You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
Orthognathic surgery is a well-established treatment for the correction of dentofacial deformities, facilitating functional and esthetic improvements. In the past two decades the procedure has evolved significantly, utilizing such advancements as virtual planning and miniplate customization to provide enhanced accuracy and safety.1-3 However, many patients and even doctors still are reluctant to employ this treatment because of its reputation of being a complex operation with intense postoperative morbidity.
Minimally invasive procedures are currently trending in all medical fields, and several recently published articles have applied this concept to orthognathic surgery. These publications have focused mainly on the modified surgical techniques used and the potential benefits that can be attained in the short-term recovery.4-6
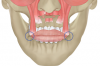
Although orthognathic surgery was first established for the purposes of correcting functional problems, the number of patients whose primary motivation is esthetic improvement has increased dramatically. The aim of this article is to describe the potential long-term esthetic benefits of the relatively new concept of minimally invasive orthognathic surgery (MIOS) (Figure 1 through Figure 3). The MIOS protocol utilizes modifications of traditional maxillary Le Fort I (LFI) osteotomy, bilateral sagittal split osteotomy (BSSO), and genioplasty procedures. Differences between MIOS and the various traditional techniques are highlighted.
Maxilla
Lip Fibrosis
That an incision results in a scar is an absolute truth, and the larger the incision, the larger the scar. For a conventional LFI osteotomy, a typical incision extends between the first molars, providing full access to the maxilla. This approach will result in a fibrosis line throughout the entire upper lip, which may jeopardize the lip's movement during smiling. This is one reason for the so-called "Le Fort I lip," whereby the appearance of the upper lip is altered, and one can recognize a patient who received an LFI osteotomy.
During MIOS, a standard incision in the maxilla is approximately 2 cm long, which is normally the distance between the lateral incisors, or shorter (Figure 4 through Figure 6). This approach preserves part of the orbicularis muscle and will result in a smaller fibrosis with less interference in lip movements. The wound closure is made in two planes, with the muscles in the deep plane reattaching with absorbable multifilament suture. Closure in the superficial plane is recommended to be done with monofilament suture to accelerate soft-tissue healing and minimize swelling. This approach represents an advantage over traditional orthognathic surgery with regard to postoperative recovery and the avoidance of fibrosis formation (Figure 7 through Figure 9).1,2
Facial Expression
The main reason for using a conventional LFI technique is to obtain full access to the maxilla, thereby gaining a direct view during osteotomy creation, mobilization of the maxilla, and especially fixation. Using the traditional approach, it is possible to position four miniplates to stabilize the maxilla in its new position; however, this is achievable only through extensive subperiosteal elevation and deep-layer muscle dissection.
Superficial and deep-layer facial muscles are attached mainly through the interconnection of fibers. Release of a deep-layer muscle will affect the tension of the muscles of the superficial layer (eg, upper lip elevator and zygomaticus muscles). This can result in flattening of the upper lip, volume shift, decrease in the amount of visible vermilion, and down-turning of the oral commissures.7 This is a second reason for the aforementioned so-called "Le Fort I lip" (Figure 10 and Figure 11).
During MIOS, the dissection is limited to the paranasal area. The LFI osteotomy is performed with a tunnel approach, the maxilla is mobilized using a "twist technique" in which the insertion and rotation of a chisel promotes the down-fracture of the maxilla,4,5 and fixation is generally achieved using only two miniplates. Beyond the various inflammatory-related benefits with regard to soft-tissue preservation-eg, less blood loss, more vascularization, fewer neurosensory disturbances, and less impact to the lymphatic drainage system-MIOS also results in reduced negative impact to lip posture and facial expression because of the preservation of the deep-layer facial muscles (Figure 12 and Figure 13).7
Nasal Widening
Beyond the amount of skeletal movement, subperiosteal dissection and flap elevation play important roles in nasal alterations. During a conventional LFI approach, most muscle insertions around the anterior nasal spine and the alar base area are detached, allowing the muscles to be retracted laterally, resulting in widening of the inter-alar width and nasal base.8-10 This undesirable esthetic outcome is fairly common, and surgical techniques have been described to avoid these results, such as V-Y closure and alar cinch suturing, although their effectiveness remains controversial.11,12
After the initial flap elevation during MIOS using a minimally invasive approach, the nasal mucosa is elevated but the anterior nasal spine is never exposed, thereby maintaining the periosteal and muscle attachments. Using a piezosurgical device, the surgeon performs a "V" osteotomy at the base of the anterior nasal spine, which remains attached to the nasal septum. This subspinal technique, which was first described by Mommaerts et al in 1997, maintains the nasal sphincter muscles attached to the anterior nasal spine, thus controlling the enlargement of the nasal base9,12 and preserving upper lip form and length both in the short term (Figure 14 through Figure 17) and long term (Figure 18 through Figure 21).
Mandible
Although less information has been written describing the use of MIOS in the mandible, this less-invasive concept has also led to novel alternatives to classic BSSO designs, with shorter osteotomies requiring smaller incisions and limited soft-tissue and muscle detachment. The MIOS approach reduces postoperative morbidity, such as edema and neurosensory disturbances, and allows earlier mandibular movements. Beyond these important inflammatory-related benefits, an oblique anterior cut is performed, moving the anterior part of the osteotomy toward the mandibular angle, instead of a conventional osteotomy at the mandibular body level. This modification of the end of the inferior cut at the lower border of the mandible can result in significant esthetic improvements.13
Angle Projection
During conventional BSSO techniques the lower border osteotomy is performed around the mandibular body, splitting the mandible with the angle attached to the proximal segment with the condyle. After being repositioned, especially during counterclockwise rotations, the mandibular body gains horizontal and vertical projection, but the mandibular angle remains at its original position.
The mandibular osteotomy in the MIOS protocol is similar to the original version of the BSSO described in 1957, which was located more posterior at the ramus portion, and which today is referred to as an anterior oblique osteotomy.14 This design allows the realization of all movements that a classic osteotomy allows, requires less exposure of infra-alveolar nerve length, and limits the risk of a bad split.
Once the anterior osteotomy is modified in an oblique direction posteriorly, the mandibular angle is kept entirely attached to the distal segment. This offers advantages because the angle is mobilized together with the body of the mandible in rotational movements, allowing the elongation of both horizontal and vertical branches (Figure 22 through Figure 25).13
Mandibular Notch
Another drawback of the classic BSSO, with the ending cut made around the mandibular body, is the risk of causing a visible and palpable osseous defect on the inferior border; this is known as "notching."13,15 Although the masseter muscle and paramandibular soft tissue may mask some of the defect, notching generates an interruption of the natural jawline, leaving a bony defect that can cause patient dissatisfaction (Figure 22 through Figure 25).
The novel version of a BSSO in MIOS preserves the integrity of the basilar edge of the mandible, dislocating posteriorly the possible formation of bony defects. It avoids the creation of a palpable or visible notch, primarily because the surrounding subcutaneous tissue at this location is thicker.13
Chin
Fibrosis and Lip Ptosis
As stated earlier, the larger is the incision, the larger the scar. This is an unchanging principle. During conventional genioplasties a typical incision provides full access to the chin, sometimes with the anterior mandibular degloved, detaching the mentalis muscle insertion and causing direct or indirect interference of other facial expression muscles, such as the depressor anguli oris and labii inferioris.7 This approach will result in a fibrosis line throughout the lower lip. Moreover, a suspensory suture is needed to avoid lip ptosis due to mentalis muscle dissection, which may sometimes occur.
In a MIOS genioplasty, a short incision of approximately 1.5 cm length is sufficient to approach the chin with tunnel dissection. It is important to limit inferior dissection to keep the maximum amount of soft tissue attached to the inferior segment (Figure 3 and Figure 6). In addition to inflammatory-related benefits, this approach potentially increases the soft-tissue response to the bone repositioning, especially in asymmetric movements, avoiding fibrosis and lip ptosis (Figure 9). Again, wound closure is recommended in two planes.Discussion
Customization is presently a reality in maxillofacial surgery, including orthognathic procedures, but most studies report such surgery using conventional or even more invasive approaches. Considering that customized fixation plates are mechanically stronger than conventional ones, requiring no extra bending, plate fixation can be facilitated through the use of small incisions. Therefore, with the development of patient-specific plates, their routine application can serve as a solution for surgeons seeking to perform MIOS.1,2
As with any new technique, a learning curve is associated with MIOS, especially with regard to maxillary down-fracture and mandibular fixation with a lower bone contact area. In the authors' view, MIOS should be carefully conducted by experienced professionals and passed on to younger practitioners.
While only few studies have reported on MIOS, these less-invasive techniques have been associated with less morbidity, a lower inflammation response, and better postoperative comfort in the short term than conventional methods.4,5,10,12 A recent systematic review suggested that its application is safe, feasible, and effective.6
Additional studies are needed to confirm the esthetic considerations associated with MIOS. As the number of professionals adopting this technique increases,6 further conclusions will be able to be made, including observations of long-term outcomes, and thus a better understanding of the technique for both clinicians and patients will be attained.
About the Authors
Jonathas Daniel Paggi Claus, PhD, DDS
Private Practice, Oral and Maxillofacial Surgery, Florianópolis, Brazil
Matheus Spinella Almeida, PhD, DDS
Private Practice, Oral and Maxillofacial Surgery, Florianópolis, Brazil
Hugo José Correia Lopes, DDS
Private Practice, Oral and Maxillofacial Surgery, Florianópolis, Brazil
Asdrubal Pereira, DDS
Private Practice, Oral and Maxillofacial Surgery, Caracas, Venezuela
Nelson Leon, DDS
Private Practice, Oral and Maxillofacial Surgery, Caracas, Venezuela
Queries to the author regarding this course may be submitted to authorqueries@broadcastmed.com.
References
1. Claus JDP, Almeida MS, Zille D. Customization in minimally invasive orthognathic surgery. Advances Oral Maxillofac Surg. 2021;3:100114.
2. Swennen GRJ. Surgical efficiency and minimizing patient morbidity by using a novel surgical algorithm in orthognathic surgery. Atlas Oral Maxillofac Surg Clin North Am. 2020;28(2):95-109.
3. Claus JDP, Almeida MS, Hernández-Alfaro F. In-house hybrid technique for customization of guides and miniplates in orthognathic surgery. J Craniofac Surg. 2020;31(4):1122-1124.
4. Hernández-Alfaro F, Bueno JM, Diaz A, Pagés CM. Minimally invasive surgically assisted rapid palatal expansion with limited approach under sedation: a report of 283 consecutive cases. J Oral Maxillofac Surg. 2010;
68(9):2154-2158.
5. Hernández-Alfaro F, Guijarro-Martínez R. "Twist technique" for pterygomaxillary dysjunction in minimally invasive Le Fort I osteotomy. Int J Oral Maxillofac Surg. 2013;71(2):389-392.
6. AlAsseri N, Swennen G. Minimally invasive orthognathic surgery: a systematic review. J Oral Maxillofac Surg. 2018;47(10):1299-1310.
7. Vercruysse H Jr, Nassauw LV, Miguel-Moragas JS, et al. The effect of a Le Fort I incision on nose and upper lip dynamics: unraveling the mystery of the "Le Fort I lip." J Craniomaxillofac Surg. 2016;44(12):1917-1921.
8. Mommaerts MY, Lippens F, Abeloos JV, Neyt LF. Nasal profile changes after maxillary impaction and advancement surgery. J Oral Maxillofac Surg. 2000;58(5):470-476.
9. Mommaerts MY, Abeloos JV, De Clercq CA, Neyt LF. The effect of the subspinal Le Fort I-type osteotomy on interalar rim width. Int J Adult Orthodon Orthognath Surg.1997;12(2):95-100.
10. Hernández-Alfaro F, de Sousa Gil AP, Haas OL Jr, et al. Soft tissue management to control nasal changes after Le Fort I osteotomy [in French]. Orthod Fr. 2017;88(4):343-346.
11. Trevisiol L, Lanaro L, Favero V, et al. The effect of subspinal Le Fort I osteotomy and alar cinch suture on nasal widening. J Craniomaxillofac Surg. 2020;48(9):832-838.
12. de Sousa Gil AP, Guijarro-Martínez R, Haas OL Jr, et al. Nasolabial soft tissue effects of segmented and non-segmented Le Fort I osteotomy using a modified alar cinch technique - a cone beam computed tomography evaluation. Int J Oral Maxillofac Surg. 2020;49(7):889-894.
13. Cordier G, Sigaux N, Ibrahim B, Cresseaux P. The intermediate length BSSO: finding the balance between the classical and short designs. J Stomatol Oral Maxillofac Surg. 2020;121(1):70-73.
14. Trauner R, Obwegeser H. The surgical correction of mandibular prognathism and retrognathia with consideration of genioplasty. I. Surgical procedures to correct mandibular prognathism and reshaping of the chin. Oral Surg Oral Med Oral Pathol. 1957;10(7):677-689.
15. Raffaini M, Magri AS, Giuntini V, et al. How to prevent mandibular lower border notching after bilateral sagittal split osteotomies for major advancements: analysis of 168 osteotomies. J Oral Maxillofac Surg. 2020;78(9):1620-1626.