You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
Due to the anatomy of the maxillary sinus, particularly after the loss of maxillary molars and premolars, the posterior maxillary region often lacks the amount of bone volume needed for dental implant placement. As a result, various techniques have been developed to enlarge the bone volume in this area. These types of techniques are referred to as “sinus floor augmentation” or “sinus lifts.”
Boyne and James1 were the first to publish a report on maxillary sinus floor augmentation in 1980. They described how sinus augmentation was performed using particulate autogenous bone harvested from the iliac crest; 3 months later, blade implants were placed to support removable or fixed reconstructions. Six years later, in 1986, Tatum2 reported a lateral window technique for raising the sinus membrane, a method that also involved raising the membrane using an inferior crestal approach through the implant preparation site. Thus, the concept of sinus floor augmentation was established and confirmed in many retrospective and prospective controlled studies reviewed by Pjetursson et al3 in 2008 in an article that also suggested various surgical techniques for sinus floor elevation.
This review traces the progression of sinus floor elevation techniques from their beginnings as a major surgical treatment to a modern minimally invasive procedure.
The Biological Concept of Sinus Floor Augmentation
Sinus floor augmentation involves the relocation of the inferior border of the maxillary sinus and creation of sufficient osseous volume for implant placement. This is accomplished by separating the maxillary sinus membrane—ie, the Schneiderian membrane—from the osseous walls at the inferior potion of the maxillary sinus, and creating adequate space for bone regeneration. This new space is filled by new viable osseous tissue that is able to support dental implants. The first histologic description of this special bone formation was published in 1994 by Nishibori et al,4 who reported on the placement of autogenous bone or allogeneic demineralized freeze-dried bone grafts in the sinuses of two patients. The study noted the presence of viable osseous tissue in both treatments, thus demonstrating the bone-forming capacity of the space beneath the periosteum of the Schneiderian mucous membrane.
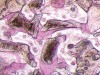
Sinus floor augmentation space may be maintained by using various autogenic, allogeneic, xenogenic, or alloplastic materials, which are utilized for guided bone regeneration procedures. The regenerative bone typically forms around the bone-filling materials (Figure 1).5 Several recent studies suggest that a blood clot alone (without filler) may also promote sufficient bone formation,6 as long as the space can be maintained during healing.
The discussion below covers the different surgical approaches to sinus floor augmentation, without addressing the different materials used.
Surgical Principle of Sinus Floor Augmentation
The basic surgical principle and technique have remained essentially the same throughout the years. After achieving intraoral access to the maxillary sinus wall through the oral mucosa, a bony window is prepared. Next, the Schneiderian membrane is dissected and raised from the sinus floor to enable insertion of a graft to facilitate bone formation in the secluded space created.
Modifications to reduce surgical complications and morbidity—both during and after the procedure—have been made in the site of access to the maxillary sinus and the extensiveness of the surgical procedure.
The two approaches used for sinus floor augmentation—the lateral approach and the crestal approach—are described below.
Lateral approach for sinus floor augmentation
The original maxillary sinus floor augmentation technique described by Boyne and James1 in 1980 was performed by osteotomy of the lateral wall of the maxillary sinus, followed by Schneiderian membrane elevation and autogenous particulate bone graft—ie, the “modified Caldwell-Luc approach.” The area was left undisturbed for 3 months to allow for sufficient healing before placement of blade implants.
Although different techniques for lateral approach sinus floor elevation have been presented since then, their differences have been minor.
The technique described below is based on a deep buccal full-thickness flap with vertical release in the canine area, followed by creation of a “window” at the lateral wall of the sinus (Figure 2). The bony window is either removed or rotated medially with the sinus membrane and pushed inward. The Schneiderian membrane is then separated from the bone anteriorly, posteriorly, and medially until clinically sufficient space is established (Figure 3). The created space, which occupies the lower third of the sinus, is filled with a bone graft (Figure 4), and the lateral access window is covered with a collagen membrane (Figure 5).
The cumulative survival rate of implants placed in augmented sinuses is 92.8%,3 and is comparable to that among implants placed in pristine maxillary bone. However, as with any surgical procedure, complications may occur during or after surgery. Perforation of the sinus membrane is the main complication associated with a maxillary sinus lift. The presence of a septum may increase the possibility of perforations. Ulm et al7 observed the presence of a septum in approximately 30% of sinuses located close to the premolar-molar region. Sinus shape, too, influences the chance of perforations. Cho et al,8 who examined different angles within the maxillary sinus, found that when the angle between the buccal alveolar wall and palatal alveolar wall was narrow, it was associated with more instances of perforations. Reporting on a simplified classification and repair system for sinus membrane perforations, Vlassis and Fugazzotto9 proposed five different classes associated with lateral window sinus lift based on their location and extent of perforation. They wrote that—depending on their extent and location—perforations that can be isolated can be repaired by folding the sinus membrane over itself and placing a collagen membrane. However, they added, when perforation continues to increase in size and cannot be isolated, the procedure should be aborted and attempted again after waiting 4 months.
Other possible complications associated with maxillary sinus augmentation may include infra-orbital nerve injury, bruising, and soft-tissue dehiscence. The risk for post-operative infections, which occur in up to 10% of sinus floor augmentation procedures, may be reduced by the use of preoperative antibiotics.10,11 Occasionally, complications such as excessive bleeding from major blood vessels near the bone of the lateral wall or the sinus membrane (Figure 6), hematomas, wound dehiscence, and implant migration into the sinus cavity are also reported to occur.12
Crestal approach for sinus floor augmentation
In 1994, Summers introduced the osteotome technique, a minimally invasive modification to sinus lift that can be used to place implants at the time of sinus surgery or to prepare a future implant placement site. Osteotome-root analog instruments are used to prepare the crestal osteotomy site (Figure 7). The osteotome is inserted through the edentulous alveolar crest at the inferior border of the maxillary sinus floor and produces a fracture at the cortical bone of the sinus floor, leaving the Schneiderian membrane intact. Then, the condensing of the bone graft material applies lateral and apical pressure, resulting in separation of the Schneiderian membrane from the floor of the sinus, creating new space for the graft between the membrane and the sinus floor.13
The osteotome technique is, by nature, a less invasive surgery with smaller flap design and a less extensive osteotomy, compared with the lateral approach for sinus floor augmentation. As a consequence, post-operative complications and morbidity are less likely to occur. In 1996, the Report of the Sinus Consensus Conference attributed 48% of failed sinus grafts to preoperative complications; among them, 38% were related to sinus-membrane perforation.14 Ferrigno et al15 reported that the rate of osteotome sinus-membrane perforation using the osteotome technique was 2.2% to 4.7%, demonstrating a significant reduction in post-surgical complications and infection associated with membrane perforation. Also with the osteotome technique, the bone volume used to augment the sinus typically averages 1 cc to 1.5 cc as opposed to 4 cc to 6 cc of bone in the lateral-window procedure. This may be particularly advantageous when the patient has a clear contraindication to lateral sinus grafting due to space-occupying masses such as polyps, retention cysts, or mucosal thickening. Also, because there is less penetration in the sinus cavity, the crestal approach also lessens the chance of osteomeatal complex obstruction, compared with the lateral window approach.
Despite its numerous advantages, the osteotome sinus lift technique is not devoid of complications. Because Summers’ osteotome technique is based on a green stick fracture of the sinus floor, damage may occur to the Schneiderian membrane. Following the osteotome technique, Krennmair et al16 reported an increased incidence of suspected membrane perforation, and Sammartino et al17 observed the occurrence of benign paroxysmal positional vertigo among approximately 3% of patients. The suspected reason for this side effect is the detachment of the otoliths from their normal location due to percussive and vibratory forces stemming from the preparation of implant bed using a surgical hammer.17 Recently, it was reported by Jensen at al18 that after the osteotome technique, a case of severe bleeding was likely due to damage to the posterior superior alveolar artery, which runs intra-sinusally in 29% of cases19 and may, therefore, readily be damaged by the osteotome.
Due to the above side effects of the osteotome technique and the patient discomfort related to the use of a surgical hammer, various modifications to the Summers technique were introduced. Cosci and Luccioli20 presented a crestal approach to sinus lift using a specific sequence of specially designed drills (Cosci technique). Each drill has a built-in ledge, and the consecutive drills were designed with stoppers in 1-mm increments to gently grind the bone of the sinus floor. The shape of the drill tip was designed to prevent perforation of the sinus membrane and permit gentle abrasive removal of the cortical bone of the sinus floor without fracture. A recent multicenter study showed that the Cosci technique results in a more than 6-mm bone gain, with a 96.3% implant survival rate.21
Since 2000, several modifications of the Cosci technique were introduced. These modifications can be divided into two aspects: modifications of the crestal osteotomy and modifications of the Schneiderian membrane elevation.
Crestal osteotomy techniques
Crestal osteotomy techniques focus primarily on drill design, cutting ability, and drill depth gauge.
Drill design and cutting ability—By the same token as the Cosci technique, different osteotomy tools were developed to diminish destructive force during creation of an access hole to the Schneiderian membrane. The Cosci technique and similar kits are based on non-cutting edge drills that gently grind bone in 1-mm step increments. This offers improved depth control of the working drills and reduced chances of damage to the Schneiderian membrane.
Other drills with characteristics similar to the Cosci drills have been suggested for crestal osteotomy. Chen and Cha22 proposed using a rounded diamond drill to create a smaller access hole to the Schneiderian membrane. Although this drill is more aggressive than those in the Cosci system, prudent preparation prevents damage to the sinus membrane. In an 8-year retrospective study, Chen and Cha22 reported more than 99% success with their technique with few side effects.
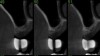
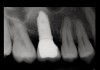
Drill depth gauge—A common complication of the crestal drill osteotomy is unintended perforation of the Schneiderian membrane. As a consequence, specific sleeves in different lengths were developed (Figure 8). These sleeves, which are placed on the drills, serve as gauge stoppers that prevent drill overextension. While the Cosci system uses only 3-mm-diameter drills, the newer systems include wider-diameter drills, which offer better visibility and control of the osteotomy and the integrity of the Schneiderian membrane. Figure 9 shows an implant insertion case using one of the newer systems to perform this crestal osteotomy technique. Osteotomy was performed with a non-cutting drill in 1-mm depth increments using depth gauge stoppers until the bone tissue is removed and the intact Schneiderian membrane is visible. The Schneiderian membrane is then elevated using bone-filling material, as described by Summers’ original technique (Figure 10). Following sufficient augmentation, the implants are inserted (Figure 11). Cone-beam computed tomography after 6 months reveals the bony mantle covering the inserted implants (Figure 12).
Schneiderian Membrane Elevation Techniques
Once access to the Schneiderian membrane is established, the membrane must be separated from the inferior border of the maxillary floor. For this, there are special tools and techniques including micro-curettes and Schneiderian membrane condensing techniques using filler or saline.
Micro-curettes— The limited access through the crestal osteotomy has led to development of various specific tools for this task. Elevation of the Schneiderian membrane in the lateral approach for sinus floor augmentation is done with special curettes, which are designed with a gentle rounded cutting edge and a non-cutting back surface. Similarly, micro-curettes were developed for the crestal approach. These mushroom-like curettes are shaped like a dome with different diameters; they enable a gentle separation of the Schneiderian membrane with minimal possibility for damage to the membrane, particularly when one of the following is used: micro-surgical suction tips, high-powered magnification loops, and direct light. These curettes, however, offer limited access to the Schneiderian membrane and are restricted in their ability to elevate the membrane. As a result, other methods to further elevate the sinus membrane must be used after these curettes.
Schneiderian membrane condensing techniques
Using bone fillers—As originally described by Summers, most crestal sinus floor augmentation techniques use bone-filling materials to push gently the Schneiderian membrane from the sinus floor through the osteotomy site. It is believed to cause even pressure, which leads to symmetrical and homogenized elevation of the membrane. However, the Schneiderian membrane has elastic properties and the tissue may have inconsistent thickness. These properties may affect the uneven pressure distribution. Furthermore, the anatomy of the sinus floor may also play a role, and concaved floor anatomy may react differently than a convex floor anatomy. The use of bone fillers diverts from the basic principle of Pascal’s law (see below), and may produce uneven pressure. Furthermore, the bone-filling particles may induce micro-tears of the membrane. A recent retrospective long-term study from the authors’ department showed that implant survival following crestal sinus floor augmentation was high and was not affected by the bone-filling material that was used, implant type, or implant diameter (unpublished results).
Using saline—The use of saline to push the Schneiderian membrane in a coronal position is based on Pascal’s law (which is also known as the principle of transmission of fluid pressure). According to this law, the pressure exerted in a confined incompressible fluid is transmitted equally in all directions throughout the fluid. Compared to bone-filling materials, the force caused by saline on the sinus membrane is distributed equally, and therefore probably results in less chance for membrane tears. Secondly, unlike particulate materials, saline might leak into the oral cavity during the injection and will lead to reduced pressure on the Schneiderian membrane. Therefore, when using saline to elevate the sinus membrane, it is essential to properly seal the osteotomy opening. Another advantage of using saline is that if membrane tear occurs, the leak of saline to the sinus cavity is less problematic than bone-grafting material. Figure 13 presents a case of crestal sinus lift using saline. A special injection tool with a silicon sealer is placed on the osteotomy opening with light pressure to provide sufficient seal of the osteotomy area, and saline is gently injected, following by appropriate filler (Figure 14 and Figure 15). Kao and DeHaven23 presented a controlled hydrostatic sinus elevation technique with saline and the use of pressure gauge. In their article, membrane elevation was carried out in a controlled manner in order to reduce chances for membrane perforation.
Using a balloon—In 2006, Kfir et al24 presented a new method to elevate the Schneiderian membrane. The idea is based on the same principle as catheterization of the coronary vessels, using liquid pressure inside a balloon to detach the Schneiderian membrane from the sinus floor (Figure 16 through Figure 19). The equipment includes a small balloon attached to an insertion tube, which is placed inside the osteotomy preparation (Figure 17). The balloon is then inflated with saline until sufficient volume is created. Following deflation and removal of the balloon, bone-filling material is inserted into the created space, and implants may be placed if anatomic conditions allow. A pressure gauge may be added to this technique and allows better control of the force inflicted on the Schneiderian membrane. In a cadaver study,25 the Summers condensation technique was compared with the balloon technique. Sinus elevation capacity was similar between the two groups. However, the incidence of membrane tears was greater in the Summers technique group, indicating reduced risk for side effects using the balloon. Recently, Mazor et al26 presented a case series using a flapless approach to the balloon technique and found 100% implant survival over 18 months follow-up.
Conclusions
The posterior region in the maxilla sometimes lack sufficient bone volume for implant insertion due to the proximity to the maxillary sinus. As a consequence, various techniques were developed in order to augment the osseous volume in these areas. Initially, major surgical approaches were designed, such as the lateral window approach, which was based on the Caldwell-Luc approach. These methods however, had relatively high incidence of complications and morbidity. Over time, less invasive methodologies were developed. The crestal approaches for sinus floor augmentation lead to reduced morbidity and complications, with success rates similar to the lateral approach. These techniques require micro-surgical skills and equipment, due to the limited access and visibility. Various techniques for crestal approach are available, and most of them show predictable results. Guidelines for choosing the right approach for this procedure is are based mostly on personal experience and the skills of the surgeon.
About the Authors
David Polak, DMD, PhD
Department of Periodontology, The Hebrew University-Hadassah Faculty of Dental Medicine, Jerusalem, Israel
Lior Shapira, DMD, PhD
Department of Periodontology, The Hebrew University-Hadassah Faculty of Dental Medicine, Jerusalem, Israel
REFERENCES
1. Boyne PJ, James RA. Grafting of the maxillary sinus floor with autogenous marrow and bone. J Oral Surg. 1980;38(8):613-616.
2. Tatum H Jr. Maxillary and sinus implant reconstructions. Dent Clin North Am. 1986;30(2):207-229.
3. Pjetursson BE, Tan WC, Zwahlen M, Lang NP. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. J Clin Periodontol. 2008;35(8 suppl):216-240.
4. Nishibori M, Betts NJ, Salama H, Listgarten MA. Short-term healing of autogenous and allogeneic bone grafts after sinus augmentation: a report of 2 cases. J Periodontol. 1994;65(10):958-966.
5. Chackartchi T, Iezzi G, Goldstein M, et al. Sinus floor augmentation using large (1-2 mm) or small (0.25-1 mm) bovine bone mineral particles: a prospective, intra-individual controlled clinical, micro-computerized tomography and histomorphometric study. Clin Oral Implants Res. 2011;22(5):473-480.
6. Riben C, Thor A. The maxillary sinus membrane elevation procedure: augmentation of bone around dental implants without frafts—a review of a surgical technique. Int J Dent. 2012;2012:105483.
7. Ulm CW, Solar P, Gsellmann B, et al. The edentulous maxillary alveolar process in the region of the maxillary sinus—a study of physical dimension. Int J Oral Maxillofac Surg. 1995;24(4):279-282.
8. Cho SC, Wallace SS, Froum SJ, Tarnow DP. Influence of anatomy on Schneiderian membrane perforations during sinus elevation surgery: three-dimensional analysis. Pract Proced Aesthet Dent. 2001;13(2):160-163.
9. Fugazzotto PA, Vlassis J. A simplified classification and repair system for sinus membrane perforations. J Periodontol. 2003;74(10):1534-1541.
10. Ewers R. Maxilla sinus grafting with marine algae derived bone forming material: a clinical report of long-term results. J Oral Maxillofac Surg. 2005;63(12):1712-1723.
11. Bornstein MM, Chappuis C, von Arx T, Buser D. Performance of dental implants after staged sinus floor elevation procedures: 5-year results of a prospective study in partially edentulous patients. Clin Oral Implants Res. 2008;19(10):1034-1043.
12. Ridaura-Ruiz L, Figueiredo R, Guinot-Moya R, et al. Accidental displacement of dental implants into the maxillary sinus: a report of nine cases. Clin Implant Dent Relat Res. 2009;11(1 suppl):e38-e45.
13. Summers RB. A new concept in maxillary implant surgery: the osteotome technique. Compendium. 1994;15(2):152, 154-156.
14. Jensen OT, Shulman LB, Block MS, Iacono VJ. Report of the Sinus Consensus Conference of 1996. Int J Oral Maxillofac Implants. 1998;(13 suppl):11-45.
15. Ferrigno N, Laureti M, Fanali S. Dental implants placement in conjunction with osteotome sinus floor elevation: a 12-year life-table analysis from a prospective study on 588 ITI implants. Clin Oral Implants Res. 2006;17(2):194-205.
16. Krennmair G, Krainhofner M, Schmid-Schwap M, Piehslinger E. Maxillary sinus lift for single implant-supported restorations: a clinical study. Int J Oral Maxillofac Implants. 2007;22(3):351-358.
17. Sammartino G, Mariniello M, Scaravilli MS. Benign paroxysmal positional vertigo following closed sinus floor elevation procedure: mallet osteotomes vs. screwable osteotomes. A triple blind randomized controlled trial. Clin Oral Implants Res. 2011;22(6):669-672.
18. Jensen SS, Eriksen J, Schiodt M. Severe bleeding after sinus floor elevation using the transcrestal technique: a case report. Eur J Oral Implantol. 2012;5(3):287-291.
19. Kang SJ, Shin SI, Herr Y, et al. Anatomical structures in the maxillary sinus related to lateral sinus elevation: a cone beam computed tomographic analysis [published online ahead of print December 8, 2011]. Clin Oral Implants Res. doi: 10.1111/j.1600-0501.2011.02378.x.
20. Cosci F, Luccioli M. A new sinus lift technique in conjunction with placement of 265 implants: a 6-year retrospective study. Implant Dent. 2000;9(4):363-368.
21. Bernardello F, Righi D, Cosci F, et al. Crestal sinus lift with sequential drills and simultaneous implant placement in sites with <5 mm of native bone: a multicenter retrospective study. Implant Dent. 2011;20(6):439-444.
22. Chen L, Cha J. An 8-year retrospective study: 1,100 patients receiving 1,557 implants using the minimally invasive hydraulic sinus condensing technique. J Periodontol. 2005;76(3):482-491.
23. Kao DW, DeHaven HA Jr. Controlled hydrostatic sinus elevation: a novel method of elevating the sinus membrane. Implant Dent. 2011;20(6):425-429.
24. Kfir E, Kfir V, Mijiritsky E, et al. Minimally invasive antral membrane balloon elevation followed by maxillary bone augmentation and implant fixation. J Oral Implantol. 2006;32(1):26-33.
25. Chan HL, Oh TJ, Fu JH, et al. Sinus augmentation via transcrestal approach: a comparison between the balloon and osteotome technique in a cadaver study [published online ahead of print June 21, 2012]. Clin Oral Implants Res. doi: 10.1111/j.1600-0501.2012.02506.x.
26. Mazor Z, Kfir E, Lorean A, et al. Flapless approach to maxillary sinus augmentation using minimally invasive antral membrane balloon elevation. Implant Dent. 2011;20(6):434-438.