You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
Among the accepted requirements for long-term maintenance and performance of implant cases are the use of properly matched components (eg, abutments, connections, abutment/implant screws), the precise fit of those components, and sufficient preload on the implant screws. Adhering to such requisites helps ensure that implant components will not need to be retrieved or disassembled, screws will not loosen, and the implants themselves will not fracture once placed. In fact, abutment screw loosening has been cited as among the most common causes of implant-supported restoration failure, after osseointegration failure.1,2
Ensuring fulfilment of these requirements becomes easier when authentic and suitably compatible components—preferably those engineered and marketed as part of the same and/or integrated implant system—are selected and used.3 Integrated and compatible implant systems typically have been engineered and designed with features and characteristics (eg, implant material, abutment-screw surface coating, connector form/size/shape) that complement and work synergistically to enhance strength, preload, flexural strength, fracture resistance, etc.3-5
Conversely, using aftermarket implant components or those not explicitly manufactured for use with the other specific and intended components could result in unpredictable sequelae that negatively impact implant treatment outcomes.3 Research has indicated that interchangeability among various brands of implant system components and third-party and/or aftermarket implant components varies.6 Although some brands might be compatible,7 they are not completely interchangeable or capable of reproducing the intimate fit and connection accuracy of the originally intended brand components.6
Implant Material Strength
When Professor Per-Ingvar Brånemark introduced dental implants more than 35 years ago, the implants, abutments, and abutment screws were manufactured from CP1 titanium, while prosthetic screws were composed of gold alloy. Today’s implants are typically made from CP4 titanium, and other implant system components are composed of titanium alloy. As a result, modern implant systems deliver significantly greater strength throughout all the components in the system as a whole (Table 1).
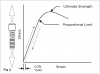
Greater strength throughout an implant system’s components is significant to placement and functional longevity and is best understood in the context of tensile stress testing (Figure 1). When implant materials undergo stress versus strain, elastic deformation occurs, in which a material is stretched under pressure, or load.8 Once the load is removed, the material returns to its original shape. However, stretching implant materials beyond their proportional limits (ie, plastic deformation) must be avoided; overtightening an abutment screw with too much torque could lead to excessive preload and screw-head fracture.2 The higher the material strength, the higher its proportional limit.8
Modern CP4 titanium implants achieve their high strength values as a result of the processes with which they are manufactured: cold working. Large-diameter bars of material are run through a series of dies and formed into narrower-diameter bars, ultimately producing an elongated grain structure with 750 MPa of strength. Annealing the material in an oven, on the other hand, maintains the original grain structure, yielding a strength of only 480 MPa.
Abutment Screw Preload
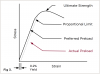
Abutment screws function similar to very stiff springs, and the abutment material can influence the strength and stability of the abutment’s connection with the implant.9 When the proper amount of torque is applied to the abutment screw, it is stretched within the previously mentioned elastic deformation zone (Figure 2).
Preload is the amount of clamping force established when the abutment screw is tightened, and this force holds the abutment intimately to the implant, which is essential for implant performance. Ideally, the abutment screw should be stretched as much as possible. Inadequate preload has been shown to result in screw loosening and poor fatigue performance of the abutment/implant complex, while excessive preload is associated with fracture.2,10 According to engineering principles, the preferred preload for screws of this type—as well as for rigid (ie, metal-to-metal) joints—is approximately 75% of the yield strength of the material.11 Such a high preload improves fatigue resistance of the connection and the locking effect. With the implant materials available today, abutment screws can be tightened 2.9 times tighter than when they were first introduced (Table 2).2,3,10
This may partially explain why original studies investigating implants cited such complications as screw loosening and screw fracture. Today’s higher-strength materials, therefore, help to ensure lower incidences of screw loosening and screw fracture, and the importance of high-strength materials to implant dentistry cannot be overstated.
However, although the desired abutment screw preload is 75% of the material strength, a problem with titanium abutment screws is the material’s very high coefficient of friction; the coefficient of friction is among the factors that influence torque efficiency and preload.12 As a result, placing a titanium abutment screw into a titanium implant causes most of the torque to produce friction rather than preload (ie, only 34% of the yield material strength in preload—results of bench testing performed by the author with 2-mm abutment screws tightened to 35 Ncm) (Figure 3).13
Issues with the effects of the coefficient of friction on preload subsequently led to the development of integrated surface coatings and surface treatments that would maximize the combination of abutment and implant materials and design in order to prevent abutment screw loosening.3,14 Other goals included diminishing the coefficient of friction and increasing preload.12
Surface Coating
In particular, research was undertaken to determine the ideal abutment and implant materials and surface coatings that would yield higher preloads on the abutment screws by lowering the coefficient of friction on the screw threads and under the screw head when the same amount of torque was applied. The preload on coated titanium abutment screws was much higher than for standard titanium screws, even after repeated tightening, loosening, and retightening (Figure 4).15 In fact, preload strength increased for the coated titanium screws after repeated loosening and tightening. Other research indicated similar preload results for abutment screws coated with tungsten carbide carbon compared with noncoated titanium alloy abutment screws.16
This type of phenomenon has been attributed to the manner in which the coating is forced into the microgaps in the threads as the screw is tightened into its compatible implant. This enhances performance and fatigue life of the overall integrated implant system.3
However, if a seemingly compatible yet different titanium screw without the appropriate surface coating is used, a much lower preload is realized, which lowers the occlusal load required to rock and lift the abutment during patient function. This ultimately results in screw loosening and compromises the integrity and strength of the implant system overall.3
Connection Types
Initially, original implant systems were predominately external hex connections. With this type of connection, the preload on the screw is significant, because the preload on the screw combined with the implant radius must be sufficient to resist the entire occlusal force placed on the implant (Figure 5). In other words, screw loosening of external hex-connected implants does not result from rotation of the abutment on top of the implant, but rather from the type of rocking that occurs when a patient functions naturally (Figure 6).
Since their introduction, however, implant connections have evolved to include internal tri-lobe and conical connection locking taper connections (Table 3). Internal tri-lobe connections feature a long skirt that fits down inside the implant. Should the occlusal force reach a level that will cause the abutment to rock, the skirt contacts the side implant wall to resist the rocking motion.
Conical connection locking taper (ie, internal hex) connections create a very intimate fit between the abutment and the implant that is critical for transferring load to the implant. By microscopically expanding the implant via the locking taper mechanism of the abutment screw when torqued, a strong, tight, and microgap-free connection is created that prevents screw loosening.4,5 This approach also enables smaller connections (eg, 3-mm narrow platform implants) for a wider variety of indications.
Implant Design
Given the intricate, complementary relationship among implant components, manufacturers strive to balance all aspects of implant system design to ensure that requisite characteristics (eg, fatigue strength, fracture resistance) are achieved. In particular, this is imperative for the implant system to demonstrate sufficient strength and stability for long-term service and restoration for patients.
Design and testing of system components begins with the implants themselves and proceeds to the abutments and connections.4,5 The wall thickness of implants must be designed sufficiently to withstand the fatigue stresses placed on the implant. This helps to prevent it from fracturing inside the mouth, which would subsequently require removal, grafting, replacement, and additional treatment time to enable the patient to return to a functioning implant. In addition, considering that today’s esthetic demands often necessitate the use of highly esthetic materials, implant components (eg, conical connections) also must be large enough to accommodate abutments manufactured from metal-free materials (eg, zirconia) and distribute the load onto the implant. By transferring and leveraging the high strength of the conical connection/abutment into the implant, the system will be able to withstand mastication forces.4
Therefore, maintaining the integrity of internal conical connections when tightening the implant into the mouth is crucial. If the wrenching/indexing feature of the hex connection is distorted in any way, subsequent procedures (eg, impression copings, final abutment placement) may be imprecise due to movement, ultimately resulting in discrepancies and inaccuracies in implant-level impressions, models, contacts, and final restorations.17 For this reason also, manufacturers of completely engineered and integrated implant systems conduct research, perform ongoing tests, and subtly modify abutments, connections, and implants to strengthen the system and ensure the overall integrity.4,5 Because the implants and connections must withstand insertion torque forces, emphasis is placed on enhancing and testing the torque strength of implants and internal hex connections.
Combining Nonintegrated Implant Components
As documented and published in the literature throughout the years, the success and integrity of implant systems are specific to the implants and components that were evaluated and tested in combination with each other in their intended manner.18 Therefore, their value and predictability, as demonstrated through laboratory and clinical testing, may not be transferable to seemingly similar products—or even the same products—if they are placed with other implants or components not specifically manufactured with the same materials, under the same conditions, or according to the same performance parameters.3,5
For example, when a standard 4.3-mm tri-lobe implant with a fatigue strength of 320 N was tested with a third-party 4.3-mm abutment, the strength of the system overall decreased to 85% of 320 N. Similar observations were made when a narrow-platform abutment from the same third-party company was placed onto a platform-switch implant system (ie, 4.3-mm narrow-platform connection). During testing, the strength of the combined system was only 55% of what had been previously achieved with the integrated system components; the implant system performance and strength fell dramatically to an unsatisfactory level.3 The clinical and long-term implications of such shortcomings can be potentially catastrophic for implant treatments.
Many reasons explain why third-party (ie, aftermarket) implant components do not perform as well as those designed, engineered, and manufactured to integrate with a specific implant system. The sample size used for reverse engineering the components (eg, abutment, connection, implant) may have been too small to ensure a quality measurement and accurate tolerances. In addition, the equipment used to measure the components may not demonstrate equivalent precision. The third-party manufacturer also has no knowledge of the material specifications and exact tolerances used by the original equipment manufacturer.
Conclusion
Among the requirements for long-term stability and predictability with implant treatments is using properly matched and integrated implant system components, achieving the proper preload, and ensuring a precise fit between the implant and abutment.3 Correctly matched components are designed for the entire implant system (eg, machined titanium, zirconia) and engineered to demonstrate a precise and accurate fit, without requiring laboratory modification. Achieving the proper preload on implant and abutment screws further requires the use of the appropriate torque wrench and matching screws to realize 35 Ncm of torque, or whatever the given manufacturer advocates and recommends.1 Combined, using properly matched components and achieving the proper preload contributes to a precise and accurate fit.
Precision, however, is also predicated on maintaining the integrity of the manufacturing process. Therefore, dentists need to use a magnification loop when inspecting abutments and implant frameworks they receive from laboratories, as well as a verification jig, to ensure that original machine lines remain visible and, ultimately, that a high-quality fit between the implant components will be established, respectively. Milled implant components have been found to be smoother than cast components, contributing to a more intimate fit between implant components; surface roughness has been correlated with microgap width.18 If the manufacturer’s machine lines have been polished and/or grit blasted away, an intimate fit cannot be guaranteed, and constant screw loosening may result.
Disclosure
Steve Hurson is a paid consultant for Nobel Biocare.
About the Author
Steve Hurson
Former Chief Scientist
Nobel Biocare
Yorba Linda, California
Queries to the author regarding this course may be submitted to authorqueries@aegiscomm.com.
References
1. Krishnan V, Tony Thomas C, Sabu I. Management of abutment screw loosening: review of literature and report of a case. J Indian Prosthodont Soc. 2014;14(3):208-214.
2. Doolabh R, Dullabh HD, Sykes LM. A comparison of preload values in gold and titanium dental implant retaining screws. SADJ. 2014;69(7):316-320.
3. Hurson S. Understanding the integrity of implant system design. Nobel Biocare website. January 18, 2011. https://www.nobelbiocare.com/us/en/home/company/media---news/articles/research-and-development/understanding-the-integrity-of-implant-system-design.html. Accessed June 1, 2016.
4. Steinebrunner L, Wolfart S, Ludwig K, Kern M. Implant-abutment interface design affects fatigue and fracture strength of implants. Clin Oral Implants Res. 2008;19(12):1276-1284.
5. Wiskott HW, Jaquet R, Scherrer SS, Belser UC. Resistance of internal-connection implant connectors under rotational fatigue loading. Int J Oral Maxillofac Implants. 2007;22(2):249-257.
6. Zanardi PR, Costa B, Stegun RC, et al. Connecting accuracy of interchanged prosthetic abutments to different dental implants using scanning electron microscopy. Braz Dent J. 2012;23(5):502-507.
7. Dellow AG, Driessen CH, Nel HJ. Scanning electron microscopy evaluation of the interfacial fit of interchanged components of four dental implant systems. Int J Prosthodont. 1997;10(3):216-221.
8. Jörn D, Kohorst P, Besdo S, et al. Influence of lubricant on screw preload and stresses in a finite element model for a dental implant. J Prosthet Dent. 2014;112(2):340-348.
9. Jo JY, Yang DS, Huh JB, et al. Influence of abutment materials on the implant-abutment joint stability in internal conical connection type implant systems. J Adv Prosthodont. 2014;6(6):491-497.
10. Xia D, Lin H, Yuan S, et al. Dynamic fatigue performance of implant-abutment assemblies with different tightening torque values. Biomed Mater Eng. 2014;24(6):2143-2149.
11. Shigley JE. Mechanical Engineering Design. New York, NY: McGraw-Hill, Inc; 1977.
12. Bulaqi HA, Mousavi Mashhadi M, Geramipanah F, et al. Effect of the coefficient of friction and tightening speed on the preload induced at the dental implant complex with the finite element method. J Prosthet Dent. 2015;113(5):405-411.
13. Data on file. Nobel Biocare. 1996. Zurich, Switzerland.
14. Basilio Mde A, Butignon LE, Arioli Filho J. Effectiveness of screw surface coating on the stability of zirconia abutments after cyclic loading. Int J Oral Maxillofac Implants. 2012;27(5):1061-1067.
15. Vizer T, Maia C, Fuchs F, et al. Development of a test model to evaluate the pre-load of screw-retained dental implant systems. European Cells and Materials. 2014;27 suppl 2:16.
16. Park JK, Choi JU, Jeon YC, et al. Effects of abutment screw coating on implant preload. J Prosthodont. 2010;19(6):458-464.
17. Gracis S, Michaelakis K, Vigolo P, et al. Internal vs. external connections for abutments/reconstructions: a systematic review. Clin Oral Implants Res. 2012;23 suppl 6:202-216.
18. Fernández M, Delgado L, Molmeneu M, et al. Analysis of the misfit of dental implant-supported prostheses made with three manufacturing processes. J Prosthet Dent. 2014;111(2):116-123.