You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
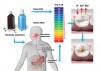
The surfaces of teeth are in a state of dynamic ion exchange in order to maintain equilibrium between demineralization and remineralization.1 On one side are factors that disrupt this balance, including acids and unhealthy habits (such as cola swishing and fruit mulling), and on the other side are factors that protect tooth-surface integrity such as fluoride and good quantity and quality of saliva (Figure 1).2,3 A change in this equilibrium toward the destructive factors can result in tooth-surface loss.4
The gradual loss of tooth structure due to acid dissolution and/or chelation without any microbial involvement is referred to as dental erosion.3 As mentioned above, this non-carious tooth lesion of multifactorial etiology can be a result of the tooth-surface ionic imbalance.5 The tooth-surface loss can be exacerbated when other conditions like dental attrition or abrasion occur simultaneously with the chemical process.6 Non-carious loss of tooth structure is shown to be on the rise in the general population due to changes in dietary and behavioral habits.7
Sources of the acid that lead to tooth erosion can be either intrinsic (acid content from within the body) or extrinsic (from an external acid source).5,8 One source of acid that is often overlooked is that of the various medications prescribed by doctors. Some medications cause dental erosion directly, as a result of their acidity or chelating action,9 while others cause erosion of the dental hard tissue secondary to their side effects (Figure 2).10 Therefore, oral healthcare providers should educate patients and colleagues about the drugs that can cause dental erosion, either directly or indirectly.
Hence, the purpose of this review is to give a broader perspective on the various therapeutic medications that can cause dental erosion. This article also aims to highlight different measures that can be taken to reduce the incidence of such an occurrence.
Direct Association
Medications with a pH of <5.5—which is the critical pH for enamel—may cause dental erosion.11 Other factors that influence the erosive potential of a substance are its titratable acidity, pKa value, chelation property, mineral content, and the time and frequency of acid contact.5Various therapeutic medications or agents have the potential to cause erosive dental lesions due to their inherent acidity. These include the following:
Vitamin C and other oral supplements: Supplemental vitamin C (L-ascorbic acid) can be dispensed as chewable tablets, syrups, or effervescent tablets.9 Prolonged use of vitamin C supplements, especially the chewable tablets, has been reported to cause severe dental erosion.12 Iron tonic and amino-acid supplements (Figure 3), too, have been implicated in tooth erosion.13
Aspirin: Prolonged use of chewable or powdered aspirin (acetylsalicylic acid) for the treatment of chronic pain has been shown to cause dental erosion.14,15 The contact time of this acidic medication with the teeth is prolonged when using chewable or powdered formulations. This, in turn, increases the risk for dental erosion.
Hydrochloric acid (HCl): Preparations containing HCl, dispensed in tablet or liquid form, may be prescribed for patients with certain gastric disorders. These are known to cause erosion of teeth, especially when chewed or swished around, rather than immediately swallowed.16
Asthma medications: Though some investigators revealed no clear association between asthma and dental erosion,17 various other studies have shown that patients with asthma are at a heightened risk of developing dental erosion.18-20 The acidic nature of the medications used to control asthma has been implicated as a reason. It has been shown that many asthmatic drugs in current use (eg, beclomethasone dipropionate, fluticasone, salmeterol, and terbutaline sulfate)—especially those delivered in the powdered form—have a pH less than the critical level of 5.5 required for the dissolution of hydroxyapatite.21 Although a study by Tootla et al22 demonstrated no clinically significant acidogenic response with the different inhalers tested, a fall in the salivary and plaque pH was seen with a lactose-based dry powder inhaler. Use of these agents multiple times in a day may erode the teeth they contact.21 The indirect association of asthmatic medications and dental erosion (reduced acid clearance and increased gastric reflux) will be discussed later.
Low-pH mouth rinses: Some of the proprietary mouth rinses available for purchase by the general public are shown to be acidic.23 Results of a study that measured the erosive potential of various low-pH mouth rinses indicated that acidified sodium chlorite mouth rinse produced erosion similar to orange juice.24 In another in vitro study, an EDTA-containing anti-calculus rinsing solution exhibited dissolution of enamel after 2 hours of exposure due to the calcium-chelating action of EDTA.25 An essential-oil mouthwash (Listerine®, Johnson & Johnson, www.listerine.com) was shown in a longitudinal in vitro study using quantitative light-induced fluorescence to cause erosion compared to the negative control, but this was only significant after 14 hours of continuous use.26 This suggests that prolonged use of these low-pH oral rinses has the potential to cause dental erosion.
Liquid medications/pediatric syrups: Numerous liquid oral medications/pediatric syrups prescribed by physicians have been shown to be acidic.27 When these acidic liquid medications are consumed for prolonged periods, as seen in cases of chronic diseases, they can cause dental erosive lesions.28 Acids—commonly citric acid—are in these medications for various reasons, including to maintain chemical stability, to control tonicity, to ensure physiological compatibility, and to improve flavor for patient acceptance.29
Medications available in effervescent/dispersible form: It has also been proposed that effervescent/dispersible tablets cause erosive tooth lesions, primarily due to their use of extra acid to promote the acid-based reactions that act to disperse effervescent and dispersible tablets on contact with water.27
Acidic salivary substitutes/salivary flow stimulants: Patients suffering from xerostomia may be advised to use either salivary flow stimulants or salivary substitutes. Salivary flow stimulants and artificial saliva with low pH and high titratable acidity can lead to dental hard tissue demineralization, especially in patients with reduced salivary protection.30
Bleaching agents: Some bleaching agents available in the market have an acidic pH. This is mainly to avoid their degradation and thereby increase storage time. It was observed in an in vitro study that acidic bleaching agents resulted in significantly higher enamel hardness loss when compared to less acidic agents.31 The presence of saliva can eliminate the demineralization effect caused by low pH.32 Therefore, it is important to consider the bleaching agent’s pH and composition, especially when treating patients with reduced salivary secretion.33
Indirect Association
The medications that have the potential to cause erosion of the dental hard tissue secondary to their side effects are mentioned below:
Drug-induced hyposalivation: Saliva plays an essential role in preserving the surface integrity of dental hard tissues. The protective role of saliva against dental erosion can be attributed to the following factors:34,35
• Dilution and clearance of erosive agents from the oral cavity
• Buffering and neutralization of acids
• Reduction of demineralization and enhancement of remineralization by the presence of calcium, phosphate, and fluoride ions
• Formation of a protective diffusion barrier (acquired pellicle) on the tooth surface
Therefore, the medications that cause reduced salivary flow can put the patient at risk of tooth erosion by reducing the protective function of saliva against extrinsic as well as intrinsic acids (Figure 4). Some of the drugs associated with reduced salivation are alpha-receptor antagonists; anticholinergics; antidepressants (eg, serotonin agonists or noradrenaline and/or serotonin re-uptake blockers); antipsychotics such as phenothiazines; atropinics; muscarinic receptor antagonists; HIV protease inhibitors; and antiasthmatic agents (beta-2 adrenoceptor agonists).10 An article on drug-induced dry mouth by Scully36 is a useful resource for additional details.
Drug-induced gastroesophageal reflux: Drugs likely to cause gastroesophageal reflux disease can cause the intrinsic gastric acid to reach the oral cavity and thus increase the risk for dental erosion.10 Some examples of such medications include antispasmodic drugs (theophylline), antiasthmatic medications, anticholinergics, progesterone, and calcium channel blockers. For more information, refer to the article by Bartlett and Smith.37
Drug-induced vomiting: Drugs that induce vomiting can also be considered an indirect cause of dental erosion. For example, abuse of ipecac syrup (an over-the-counter emetic) by bulimics can result in dental erosion. Similarly, patients undergoing cytotoxic chemotherapeutic drug treatment for malignancies may suffer from frequent vomiting, resulting in erosion. Thus, extended use of such drugs can cause dental erosion as a secondary side effect.
Prevention and Management
Various measures to prevent and reduce the incidence of dental erosion related to medications have been summarized in Table 1 as The 9 Rs in the management of dental erosion.
Conclusion
Various medications can either directly or indirectly be implicated as causative factors in the etiopathogenesis of tooth erosion. It is the responsibility of dental professionals to educate patients and medical practitioners about the different precautions that can be taken to prevent and control therapeutic medication–related dental erosion.
Disclosure
The authors had no disclosures to report.
About the Authors
Manuel S. Thomas, BDS, MDS
Associate Professor
Department of Conservative Dentistry and Endodontics
Manipal College of Dental Sciences
Manipal University
Mangalore, India
A. R. Vivekananda Pai, BDS, MDS
Professor
Department of Conservative Dentistry and Endodontics
Faculty of Dentistry
Melaka-Manipal Medical College
Bukit Baru, Malaysia
Amit Yadav, BDS, MDS
Assistant Professor
Department of Conservative Dentistry and Endodontics
Manipal College of Dental Sciences
Manipal University
Mangalore, India
References
1. Smales R, Kaidonis J, Dawes C. Tooth structure, saliva and critical pH. In: Yip KHK, Smales RJ, Kaidonis JA, eds. Tooth Erosion: Prevention and Treatment. New Delhi, India: Jaypee Brothers Medical Publishers;2006:11-24.
2. Abrahamsen TC. The worn dentition—pathognomonic patterns of abrasion and erosion. Int Dent J. 2005;55(4 suppl 1):268-276.
3. Shaw L, Smith AJ. Dental erosion—the problem and some practical solutions. Br Dent J. 1999;186(3):115-118.
4. Boland TW. Dental erosion: more acid means fewer teeth. New South Wales Public Health Bulletin. 1999;10(4):35-38.
5. Lussi A, Hellwig E, Ganss C, Jaeggi T. Buonocore memorial lecture. Dental erosion. Oper Dent. 2009;34(3):251-262.
6. Addy M, Shellis RP. Interaction between attrition, abrasion and erosion in tooth wear. Monogr Oral Sci. 2006;20:17-31.
7. Lussi A. Erosive tooth wear – a multifactorial condition of growing concern and increasing knowledge. Monogr Oral Sci. 2006;20:1-8.
8. Bartlett DW. The role of erosion in tooth wear: aetiology, prevention and management. Int Dent J. 2005;55(4 suppl 1):277-284.
9. Hellwig E, Lussi A. Oral hygiene products and acidic medicines. Monogr Oral Sci. 2006;20:112-118.
10. Tredwin CJ, Scully C, Bagan-Sebastian JV. Drug-induced disorders of teeth. J Dent Res. 2005;84(7):596-602.
11. Zero DT. Etiology of dental erosion—extrinsic factors. Eur J Oral Sci. 1996;104(2):162-177.
12. Giunta JL. Dental erosion resulting from chewable vitamin C tablets. J Am Dent Assoc. 1983;107(2):253-256.
13. Yip K, Smales R, Kaidonis J. Diagnosis and control of extrinsic tooth erosion. In: Yip KHK, Smales RJ, Kaidonis JA, eds. Tooth Erosion: Prevention and Treatment. New Delhi, India: Jaypee Brothers Medical Publishers; 2006:63-68.
14. McCracken M, O’Neal SJ. Dental erosion and aspirin headache powders: a clinical report. J Prosthodont. 2000;9(2):95-98.
15. Grace EG, Sarlani E, Kaplan S. Tooth erosion caused by chewing aspirin. J Am Dent Assoc. 2004;135(7):911-914.
16. Maron FS. Enamel erosion resulting from hydrochloric acid tablets. J Am Dent Assoc. 1996;127(6):781-784.
17. Dugmore CR, Rock WP. Asthma and tooth erosion. Is there an association? Int J Paediatr Dent. 2003;13(6):417-424.
18. McDerra EJ, Pollard MA, Curzon ME. The dental status of asthmatic British school children. Pediatr Dent. 1998;20(4):281-287.
19. Al-Dlaigan YH, Shaw L, Smith AJ. Is there a relationship between asthma and dental erosion? A case control study. Int J Paediatr Dent. 2002;12(3):189-200.
20. Sivasithamparam K, Young WG, Jirattanasopa V, et al. Dental erosion in asthma: a case-control study from south east Queensland. Aust Dent J. 2002;47(4):298-303.
21. O’Sullivan EA, Curzon MEJ. Drug treatments for asthma may cause erosive tooth damage. BMJ. 1998;317(7161):820.
22. Tootla R, Toumba KJ, Duggal MS. An evaluation of the acidogenic potential of asthma inhalers. Arch Oral Biol. 2004;49(4):275-283.
23. Bhatti SA, Walsh TF, Douglas CW. Ethanol and pH levels of proprietary mouthrinses. Community Dent Health. 1994;11(2):71-74.
24. Pontefract H, Hughes J, Kemp K, et al. The erosive effects of some mouthrinses on enamel. A study in situ. J Clin Periodontol. 2001;28 (4):319-324.
25. Rytömaa I, Meurman JH, Franssila S, Torkko H. Oral hygiene products may cause dental erosion. Proc Finn Dent Soc. 1989;85(3):161-166.
26. Pretty IA, Edgar WM, Higham SM. The erosive potential of commercially available mouthrinses on enamel as measured by Quantitative Light-induced Fluorescence (QLF). J Dent. 2003;31(5):313-319.
27. Maguire A, Baqir W, Nunn JH. Are sugars-free medicines more erosive than sugars-containing medicines? An in vitro study of paediatric medicines with prolonged oral clearance used regularly and long-term by children. Int J Paediatr Dent. 2007;17(4):231-238.
28. da Silva Pierro VS, Furtado BR, Villardi M, et al. Erosive effect of an antihistamine liquid formulation on bovine teeth: influence of exposure time. Braz J Oral Sci.2010;9(1):20-24.
29. Valinoti AC, Pierro VS, Da Silva EM, Maia LC. In vitro alterations in dental enamel exposed to acidic medicines. Int J Paediatr Dent. 2011;21(2):141-150.
30. Meyer-Lueckel H, Schulte-Mönting J, Kielbassa AM. The effect of commercially available saliva substitutes on predemineralized bovine dentin in vitro. Oral Dis. 2002;8(4):192-198.
31. Magalhães JG, Marimoto AR, Torres CR, et al. Microhardness change of enamel due to bleaching with in-office bleaching gels of different acidity. Acta Odontol Scand. 2012;70(2):122-126.
32. Sa Y, Sun L, Wang Z, et al. Effects of two in-office bleaching agents with different pH on the structure of human enamel: an in situ and in vitro study. Oper Dent. 2013;38(1):100-110.
33. Araujo NC, da Costa Soares MU, Nery MM, et al. Effect of pH values of two bleaching gels on enamel microhardness. Gen Dent. 2013;61 (4):55-58.
34. Zero DT, Lussi A. Erosion—chemical and biological factors of importance to the dental practitioner. Int Dent J. 2005;55(4 suppl 1):285-290.
35. Buzalaf MA, Hannas AR, Kato MT. Saliva and dental erosion. J Appl Oral Sci. 2012;20(5):493-502.
36. Scully C. Drug effects on salivary glands: dry mouth. Oral Dis. 2003;9(4):165-176.
37. Bartlett DW, Smith BG. Etiology and management of tooth wear: the association of drugs and medicaments. Drugs Today (Barc). 1998;34(3):231-239.
38. Amaechi BT, Higham SM. Dental erosion: possible approaches to prevention and control. J Dent.2005;33(3):243-252.
39. Serra MC, Messias DC, Turssi CP. Control of erosive tooth wear: possibilities and rationale. Braz Oral Res. 2009;23(suppl 1):49-55.
40. Lussi A, Hellwig E. Risk assessment and preventive measures. Monogr Oral Sci. 2006;20:190-199.
41. Featherstone JD, Domejean-Orliaguet S, Jenson L, et al. Caries risk assessment in practice for age 6 through adult. J Calif Dent Assoc. 2007; 35(10):703-713.