You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
A common conception among many general practitioners is that the needs of their practices do not justify the purchase of a cone-beam computed tomography (CBCT) system. Beyond the financial cost, there is also concern about the risk it poses to patients in terms of radiation exposure. There are, however, significant advantages that CBCT offers general practitioners who integrate it into their armamentarium, including using the technology to generate and incorporate the vital patient information contained in its digital imaging and communications in medicine (DICOM) files, which can be merged with stereolithographic (STL) files to create multiple digital workflows.
This article will particularly emphasize how CBCT, for the first time, offers general practitioners who place implants—as an ever-increasing number are—the ability to offer their patients restorative-based implant placement. Additionally, this article will discuss the radiation risks, which are minimal—especially when compared to medical CT and even everyday environmental exposure—and explain strategies for reducing that dosage further still with collimators, low-dose settings, and confined exposure based on scout films.
Uses for CBCT
Diagnosis
General practitioners who associate CBCT with—and perhaps even use it for—root canal, tooth removal, temporomandibular joint disorder (TMJ), implant placement, obstructive airway, and orthodontic diagnosis and treatment planning may not be cognizant of how this technology can serve their practice needs in other, more practical ways. Beyond implant placement or endodontic procedures CBCT technology can be readily used in the dental office to perform common diagnostic tasks in place of traditional methods. This can be advantageous for many patients. Like panoramic x-rays, CBCT data is captured extraorally; therefore, patients may be either standing or seated while a scan is being performed, depending on what is more comfortable. CBCT data capture can especially be a preferred option with patients who find intraoral sensor placement uncomfortable. This is particularly the case with children and others who cannot tolerate having anything placed in their mouth, whether because of anatomic limitations, a sensitive gag reflex, or other reasons.
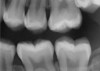
CBCT can also be used in this same manner to perform an even more common task, bitewing images, which are clinically indicated as often as every 18 to 24 months. For hygiene patients whose films require updating, CBCT offers a “patient-friendly” approach. Given that these films, which are usually performed intraorally, are often taken on an hourly basis in the typical general practice, the technology can be well utilized while also increasing comfort and satisfaction among patients. In addition, due to the expanded field of view that can be achieved with these extraoral CBCT images, they can often be more diagnostically valuable than images produced with an intraoral sensor (Figure 1 and Figure 2).
Digitizing Traditional Impressions and Models
CBCT is not necessarily appropriate for every situation. It is not intended to supplant intraoral radiography—which may be either traditional or digital—and should only be used in addition to those technologies when the 2-dimensional data gathered using them dictates the need for 3-D evaluation.1 Indeed, although CBCT scans can provide invaluable images of the maxilla and mandible, the technology has some limitations when it comes to assessing other anatomic structures, including the tooth surface.2 While intraoral scanning is becoming more prevalent in general practices, many clinicians may be reluctant, for various reasons, to convert their practices to a completely digital workflow. Therefore, general practitioners who are not currently using intraoral scanners or taking digital impressions can benefit from CBCT technology by using it to create digital versions of traditional impressions or poured models.
Typically, a traditional impression is made and sent to a laboratory, where it is often scanned using 3-D technology, then designed and milled. Clinicians who employ CBCT technology in the office can generate digital versions of traditional impressions or poured models, which then can be electronically sent to their laboratory or CAD/CAM system. Workflows for restorations, surgical templates, model fabrication, model storage, and other procedures can then be carried out. These now digital versions can be transmitted to a multitude of partners for many different types of workflows without the need for intraoral scanning.
With CBCT, clinicians can otherwise reap all the benefits of digital radiography, including the ability to enhance images and easily share the digital files with other dental team members. Furthermore, the DICOM files generated by CBCT can be used with a multitude of different software programs and merged with the commonly used STL files. In this way, digital images can be “pinned” with DICOM data. These can then be used for electronic transmission to their laboratory or CAD/CAM system, imported into their implant planning software, or otherwise placed into the digital workflow for purposes of diagnosis, treatment, electronic transmission, and communication.
Treatment Planning
From the author’s perspective, the true value of CBCT technology lies in its capacity to completely transform implant treatment planning from a “bottom-up” undertaking, where the clinician must restrict the plan to existing bone, to a “top-down” approach that focuses principally on ideal tooth placement—ie, “restorative-based” implant placement.
Although workflows can vary, in many implant cases, typically a CBCT scan of the area of concern is made. Then, with an intraoral scan or digital version of a model or impression, the practitioner begins working with the design software of the particular intraoral scan or CBCT system being used (Figure 3 through Figure 5). The edentulous area or area where teeth are to be extracted can then be thoroughly evaluated. Ideal restorations can then be previsualized or treatment planned from both an esthetic and functional standpoint. Once this is done, the intraoral information is pinned or overlaid onto the CBCT scan. The restoration(s) can then be imported into the software system, toggled on or off—ie, shown or not—and the underlying bone evaluated.3
If the ideally designed restorations cannot be supported by available bone, additional surgical procedures, such as grafting, may be indicated. Implants can be placed in 3-D in the ideal location for esthetics and function, allowing the practitioner to visualize where osseous grafting may be needed to achieve that positioning. Alternatively, implants can be virtually positioned based on the available anatomy, respecting anatomical structures such as the inferior alveolar nerve, maxillary sinus, and the buccal/lingual plates (Figure 6 and Figure 7). This restorative-driven implant placement workflow allows general practitioners to see what may be needed to augment bone to support ideal restorations. This may alert them to the need for additional surgical procedures or to open further dialogue with surgical team members.
If the intraoral scan data is not available, once the CBCT is acquired, some systems have software that uses a tooth library to place the teeth ideally in terms of function, form, and esthetics. In this way, the first priority is always determining how best to place the implant according to the restoration, as opposed to where the bone is; however, it also provides advanced notice when other procedures are needed to achieve that ideal.
Equipped with this information, the clinician is able to inform the patient of any additional time or cost that may be involved in achieving the ideal restoration, and as a result, if need be due to patient considerations such as finances or other issues, they can agree to a compromise solution—eg, in tooth position or esthetics.
An additional advantage is that other members of the dental team can quickly and easily evaluate the plan via “cloud” computing or electronic transmission of the DICOM file, and once it is approved, the team can proceed using this information to create precise surgical guides that consider both hard tissue and optimal restoration location. Using both CBCT data and intraoral scan impression or model scans, the restorations can be previsualized and the implants placed accordingly.
The Is Radiation
Much of the concern about radiation exposure from dental imaging, including CBCT, stems from the much higher dosage generated by medical CT devices, which function differently. Medical CT devices use a beam of radiation that rotates around a patient multiple times, depending upon the area being scanned, thus emitting a higher dose of radiation. They also create slices, which are then reformatted into images. In contrast, advanced dental CBCT can achieve a complete scan of the desired part of an individual’s jaw with a single quick beam that creates an image, which is then reformatted into slices.4 CBCT uses a cone-shaped beam of radiation to acquire data in a single 360-degree rotation,3 thus revealing the internal architecture of an object.5
Compared to conventional medical CT scanning, an advantage of CBCT relates to x-ray beam limitation (collimation of the primary beam) and significant dose reduction. The dose for a conventional CT, measured in microsieverts (1 μSv = 0.000001 Sv) ranges from 100 μSv to 300 μSv for the maxilla and 200 μSv to 500 μSv for the mandible, whereas CBCT ranges from 34 μSv to 102 μSv for both the maxilla and mandible together.5 The use of a thyroid collar and patient positioning modifications can reduce dosages by up to 40%. (For comparison’s sake, one recent study found that the dosing of digital panoramic units varied from 8.9 μSv to 37.8 μSv depending on the type of unit used and other factors.6) In addition, with CBCT, rapid scan times (10 to 70 seconds)5 make this method of imaging more comfortable for the patient; in contrast, medical CT scans can take 2 minutes or more to complete.
When considering the concerns about radiation exposure from dental imaging, the issue must be put into perspective. Both dentists and their patients should understand that radiation exposure is part of daily life apart from its medical and dental applications. Humans are exposed to radiation from natural materials in the earth, radon in the air, cosmic exposure from outer space, and as a result of the food and water they consume. The average dose of radiation, measured in millisieverts (1 mSv = 0.001 Sv), per person, per year from all sources is about 6.2 mSv, and international standards allow exposure to as much as 50 mSv a year for those who work with and around radioactive material.7
The National Council on Radiation Protection and Measurements places the effective radiation dose equivalent from all sources in the United States at 3.6 mSv per year, of which 3 mSv is from natural sources. And of that remaining 0.6%—most of which is medically related—only 1% is dental.8
Nevertheless, dentists should use radiographic procedures that increase patients’ radiation dose only when necessary for diagnosis and treatment and should apply the ALARA principle—as low as reasonably achievable—to reduce radiation exposure to their patients. This, according to the American Dental Association, can be done by: “determining the need for and type of radiographs to take; using ‘best practices’ during imaging, including the application of quality control procedures; and interpreting the images completely and accurately.”9
Clinicians can further minimize dose reduction by adjusting the exposure factors and limiting the field of view to the smallest dimensions consistent with the clinical situation.1 This can be achieved using a scout film—ie, a preliminary film, low-dose image, taken of a region to serve as a baseline before a definitive imaging study—before using full-volume CBCT, which emits a higher amount of radiation by volume during implant placement. Therefore, when the area is, for example, restricted to the upper left quadrant, the practitioner can use the collimator or dial down the volume.
An Investment in the Practice
It is this author’s contention that, in terms of making an investment in new technology, general practitioners who purchase a system designed to meet unique practice needs and maximize its utilization can expeditiously recoup the investment through appropriate frequent use for panoramic and bitewing images while expanding their scope of practice and increasing patient satisfaction. There is even potential to become a resource for other dental practices in the area. In addition, practitioners who have CBCT technology in their offices may not need to purchase intraoral scanners, as they can use the CBCT to scan impressions or models and send them to the laboratory for restoration fabrication.
As noted above, implant placement can be immeasurably improved using CBCT, enabling the practitioner to produce overlays of the missing teeth where the bone is and then, utilizing the captured information about the edentulous area, use the software that comes with the CBCT, the DICOM data, and imported STL files and use the tooth library to virtually place the implants and generate surgical guides. CBCT is available in a wide variety of investment levels, so practitioners considering purchasing the technology should keep their own needs in mind at all times.
Finally, from a medical–legal standpoint, practitioners are responsible for evaluating the entire scanned area, even though much of it may lie outside the area treated in the dental practice. Liability issues could potentially be raised holding dentists responsible for tumors, for example, or other abnormal findings that were not identified following a CBCT scan. With that in mind, some companies offering CBCT systems have developed limited scan units that target the area typically treated in dentistry. These may limit the potential liability of the practitioner if something is present on a scan that is not identified and reported to the patient. It is advised that practitioners review entire scans; if something does appear that looks abnormal, the patient should be referred to the appropriate medical practitioner for further evaluation.
Conclusion
Given the theoretical risks of any technology that could harm patients, practitioners should be aware of when CBCT is justified despite the radiation exposure. They should also know about the many ways CBCT aids diagnosis and treatment when not used directly on patients, such as when used to digitize traditional impressions or poured models.
In conclusion, by investing in CBCT, practitioners can offer both their patients and their dental team the significant benefits it provides. They should first, however, acquire an understanding of what this technology offers in terms of diagnosis, treatment, convenience, and patient satisfaction.
References
1. Bornstein MM, Scarfe WC, Vaughn VM, Jacobs R. Cone beam computed tomography in implant dentistry: a systematic review focusing on guidelines, indications, and radiation dose risks. Int J Oral Maxillofac Implants. 2014;29 suppl:55-77.
2. Ganz SD. The next evolution in CBCT: combining digital technologies. Inside Dentistry. 2013;9(2):116-118.
3. Zheng QH, Wang Y, Zhou XD, et al. A cone-beam computed tomography study of maxillary first permanent molar root and canal morphology in a Chinese population. J Endod. 2010;36(9):1480-1484.
4. Gutierrez N. Discovering a new dimension in dental care. UT Health Sciences Center website. http://uthscsa.edu/mission/article.asp?id=259. August 2004. Accessed June 24, 2014.
5. Shenoi RP, Ghule HM. CBVT analysis of canal configuration of the mesio-buccal root of maxillary first permanent molar teeth: An in vitro study. Contemp Clin Dent. 2012;3(3):277-281.
6. Lee GS, Kim JS, Seo YS, Kim JD. Effective dose from direct and indirect digital panoramic units. Imaging Sci Dent. 2013;43(2):77-84.
7. Radiation dose chart. American Nuclear Society website. www.new.ans.org/pi/resources/dosechart/msv.php. Accessed June 4, 2014.
8. Meyer E. Living in a radioactive world. Inside Dental Assisting. 2013;9(2). www.dentalaegis.com/ida/2013/04/living-in-a-radioactive-world. Accessed June 24, 2014.
9. Dental x-ray talking points. American Dental Association website. www.ada.org/EPUBS/assets/ememo/NYT-Cone-Beam-Talking-Points.pdf. Nov. 23, 2010. Accessed June 24, 2014.
About the Author
Curtis E. Jansen, DDS
Private Practice, Monterey, California
Queries to the author regarding this course may be submitted to authorqueries@aegiscomm.com.