You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
The loss of a single anterior tooth can be difficult for almost any patient, but replacing it with an implant or a fixed partial denture results in a predictable esthetic outcome unless significant bone and soft tissue were lost with the tooth. Even then, in the hands of a skilled team of clinicians, the result is generally acceptable. The loss of multiple anterior teeth, especially if they are adjacent to each other, is a much more difficult esthetic challenge and often requires the combination of implants and ovate pontics to achieve an acceptable esthetic result.
Height Considerations Influencing Treatment Outcome
Accounting for this difference are the biology of the periodontium and the response of the bone and soft tissues when one tooth is lost rather than multiple teeth. In the case of a single-tooth loss, if a single-tooth implant is placed, the interproximal papilla levels will be determined by the height of the interproximal bone on the adjacent natural teeth, not the interproximal bone on the implant.1-3 In the average patient, the papilla height will be 4 mm to 4.5 mm above the interproximal bone on the adjacent natural teeth (Figure 1). Therefore, if the natural teeth have no bone loss, the papilla height after tooth loss will be similar to what it was before tooth removal because the average papilla height above bone between natural teeth is also 4.5 mm.4,5 The facial gingival margin around the implant, however, is not related to the bone on the adjacent natural teeth, but rather to the facial bone levels on the implant, as well as the thickness and position of the free gingival margin before tooth removal.6,7 For a single anterior implant, the least predictable soft-tissue outcome results when the adjacent natural teeth have interproximal bone loss because managing the papilla heights can be difficult.
These same rules closely apply to the replacement of a single anterior tooth with a pontic (ie, the final papilla location will be influenced by the bone on the adjacent natural teeth, and the free gingival margin location dictated by the location of the bone and tissue thickness on the facial of the pontic). However, when comparing pontics with implants, the one significant difference concerns the height of interproximal tissue above the bone. While this height averages 4.5 mm between natural teeth, or between a natural tooth and an implant, it has been shown that after soft-tissue grafting, the amount of tissue above the bone interproximally between a pontic and a natural tooth, or between a pontic and an implant, averages 6.5 mm and, in fact, in some patients can be as high as 9 mm.8 If the adjacent natural teeth in a single-tooth replacement situation have bone loss, soft-tissue ridge augmentation, followed by placement of a pontic, can achieve greater coronal height of the papilla than a single-tooth implant could in the same situation.
Biologic Responses of Tissue in Different Locations Postextraction
The challenge of multiple tooth replacement occurs when adjacent teeth are already missing or need to be removed. Consider the loss of two maxillary central incisors. It is helpful to separate the biological response to evaluate how the soft tissue responds in several locations following tooth removal.
First, consider the response of the papilla between the centrals that were removed and the adjacent remaining lateral incisor. The same scenario exists as if the situation involved a single-tooth replacement (ie, the interproximal bone on the remaining lateral incisor will determine the papilla height between the centrals and laterals). The facial free gingival margin height on each central also will be similar in response to a single missing tooth (ie, the facial bone level and tissue thickness will determine the final facial gingival margin). In addition, just as in the single-tooth situation, if the final facial gingival margin is less than ideal, it is much easier to augment in height and thickness on both centrals with a soft-tissue procedure than it is to improve the papilla’s height.
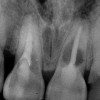
The real challenge when removing the two centrals is to evaluate what happens to the papilla between them after extraction.9,10 Before extraction, the osseous crest around both centrals, assuming no periodontal disease exists, roughly follows the scalloped nature of the cementoenamel junctions (CEJs) as they flow from the facial into the interproximal, resulting in an average osseous scallop of 3 mm; the average interproximal bone height is 3 mm coronal to the facial crest of bone. Because the soft tissue typically follows the scallop of the bone, the osseous scallop results in a gingival scallop of 3 mm. However, when teeth are present, an interesting phenomenon occurs. The gingiva on the facial of the tooth is positioned so that, on average, the free gingival margin is 3 mm coronal to the crest of bone. However, the interproximal papilla between teeth is positioned, on average, 4.5 mm coronal to the interproximal crest of bone, 1.5 mm, on average, more coronal to the crest of bone than is the facial tissue. This additional 1.5 mm, along with the 3 mm average osseous scallop, results in the tip of the papilla being an average 4.5 mm to 5 mm coronal to the facial free gingival margin (Figure 2).
Replacement Methods and Their Impact on Bone and Tissue
It is necessary to understand what happens to the osseous scallop and papillary soft-tissue height above bone following tooth removal. To a certain extent, the answer to this dilemma is determined by how the central incisors will be replaced and how the replacement method affects the underlying bone and the soft tissue.
Use of Adjacent Single Implants
Traditionally, implants have been made that are nonscalloped or flat coronally; during placement, the implant is placed apically until the platform of the implant is level with the facial crest of bone. However, because the bone is scalloped, the interproximal platform of the implant may be apical to the interproximal crest of bone by as much as 3 mm. Classically, a certain amount of bone adjacent to the implant has been expected to resorb over time, usually to the first thread of the implant.11,12 As these bony changes occur, the interproximal crest of bone that was present at the time of tooth removal might resorb, resulting in a flattening of the osseous crest and a corresponding flattening of the gingival architecture because of the papilla’s height loss as the interproximal bone is lost.
Several different approaches are currently being researched to resolve this loss of the interproximal crest of bone between implants. They include scalloped implants, platform switching, altered coronal implant surface design, and microgap location. A discussion of these approaches is beyond the scope of this article, but it bears noting that the maintenance of the interproximal crest of bone is critical to maintaining the height of the papilla between adjacent implants. In addition, there is wide concurrence that it is vital to the maintenance of the crest of bone to maintain 3 mm of space between the platforms of the adjacent implants.13 It is also necessary to understand what happens to the height of the interproximal soft tissue above the bone. While the research points to the papilla height being 4.5 mm above the bone between adjacent teeth and bone, or 4.5 mm above the bone on the natural teeth and an adjacent implant, it appears that when adjacent implants are placed, the papilla height above the bone reduces from 4.5 mm to between 3 mm and 3.5 mm.13 When adjacent implants are placed, even if they maintain the interproximal crest of bone perfectly, the papilla between the implants will end up 1 mm to 1.5 mm apical to where it was between the teeth, simply from the change in soft-tissue levels (Figure 3). If this 1-mm to 1.5-mm difference is added to any alterations in interproximal crestal bone height, it is easy to comprehend why the maintenance of the papilla height between adjacent implants is difficult (Figure 4).
Use of Pontics
The use of pontics rather than adjacent implants to replace the two centrals poses its own challenge.14 The soft tissue between the central pontics and the lateral abutments will behave similarly to that described when using a pontic to replace a single tooth, as will facial tissue. Just as it was with the adjacent implants, the concern in this instance is the papilla between the adjacent pontics. The difference, however, is that when pontics are used, it is almost guaranteed that the interproximal crestal bone between the extracted centrals will resorb, creating a flat bony ridge and a subsequent loss of papillary height. Another difference is that it is possible to augment the soft tissue between pontics significantly more above the flattened osseous crest (ie, an average of 6.5 mm) as opposed to the typical tissue above interproximal bone between adjacent implants (ie, 3 mm to 3.5 mm). Ultimately, it becomes possible to have a papilla between central pontics 3 mm more coronal than a papilla between adjacent implants for the same interproximal crest location.
Most Common Clinical Presentations
The purpose of this background information about the osseous and gingival response to removing multiple teeth is to make the clinician aware of the treatment limitations before determining a final course of action when multiple anterior teeth must be lost. It also provides a basis for predicting the treatment outcome for the four most common presentations a clinician is likely to encounter.
1. The teeth are present and need to be removed, but have no periodontal disease.
2. The teeth are present and need to be removed, and have periodontal disease.
3. The teeth are missing and the osseous and soft-tissue ridges are flattened, but the free gingival margin location on the ridge is acceptable.
4. The teeth are missing, and the osseous and soft-tissue ridges are positioned apically by a significant amount.
Possible Management options for Presentations and Their Likely Compromises
Teeth Are Present and Need Removal, but There Is No Periodontal Disease
The most predictable of all presentations is patients who need multiple teeth removed and have no periodontal disease. The challenges in these patients are usually related to whether to use implants vs a fixed partial denture and, if implants are used, how many to use and where to place them. The answers generally depend on which teeth are being removed. For example, if the two maxillary centrals are being removed and have good bone, placing adjacent implants can result in a predictable and esthetic final result; because the papilla between the central implants and the adjacent laterals will be excellent, the facial gingival margins can be easily augmented, if necessary; and the papilla between the central implants should remain within 1 mm to 2 mm of the pre-extraction papilla level, as long as the implants are placed 3 mm apart and the interproximal crest of bone is maintained (Figure 5, Figure 6, Figure 7, Figure 8 and Figure 9). In this case the patient could be treated with a fixed prosthesis using the lateral incisors as abutments. However, because the interproximal bone between the extracted centrals most likely will be lost, the risk of greater recession of the papilla between the centrals exists. Soft-tissue augmentation also would be able to create an excellent papilla in this location before completing the restoration.
If the teeth to be removed involve a central and lateral, or a lateral and cuspid, the treatment choices are not quite as clear. The challenge is twofold.
1. It is difficult to place adjacent implants in a central and lateral position, or a lateral and cuspid position, and have 3 mm between the platform of the implants. This leaves a high risk of losing the interproximal crest of bone between the implants over time, with subsequent loss of papillary height (Figure 10, Figure 11, Figure 12 and Figure 13).
2. If papillary height is lost between the central and lateral on one side while natural teeth exist on the other side, the discrepancy in papilla heights is much more noticeable than when there is a slight loss of papilla height in the middle between adjacent central incisor implants.
For these reasons, as well as the fact that the use of adjacent implants to replace a central and lateral or lateral and cuspid is unnecessary because of the lower occlusal forces in the anterior, the author almost invariably chooses to cantilever the lateral incisor as an ovate pontic off of a single central implant, or off a single cuspid implant. This is because it is esthetically more predictable and functionally as acceptable as adjacent implants.
Another option for the missing central and lateral or missing lateral and cuspid is the use of soft-tissue augmentation and a fixed prosthesis. While this can create a pleasing esthetic result, it is a more complex restoration structurally, especially when it involves the replacement of the lateral and a cuspid with pontics.
When three or four adjacent anterior teeth with good periodontal support need to be removed, the author’s preference is not to place adjacent implants, but rather separate them by one or two pontics. If both centrals and a lateral need to be removed, the author recommends placing a central implant, central pontic, and lateral implant. This design allows excellent papilla heights in all locations because of the predictability of the soft-tissue augmentation in the pontic site (Figure 14, Figure 15, Figure 16, Figure 17 and Figure 18).
If all four incisors need to be removed and good periodontal support exists, there are two acceptable options. The first is to place implants in both lateral incisor locations and use both centrals as pontics. The second is to place the implants in both central locations and cantilever the lateral incisor pontics. Both options will produce acceptable esthetic and structural results.
Teeth Are Present and Need Removal and Have Periodontal Disease
If the above scenarios present and the teeth have pre-existing bone loss, new challenges exist. Specifically, the papilla height in the areas of the periodontal disease becomes less predictable after tooth removal. This often leads to a greater degree of papillary recession and a more apically placed contact in the restorations to avoid an open gingival embrasure. In these situations, the clinician is faced with using implant restorations that will be functionally and structurally acceptable, but esthetically more difficult; or employing soft-tissue grafting and fixed partial dentures where the ability of grafting and the use of pontics can produce significantly more soft tissue over the interproximal bone (ie, 3.5 mm between adjacent implants vs 6.5 mm above bone for pontics). As a rule, the decision is based on the patient’s esthetic needs (ie, high lip line) vs the teeth’s condition. If the adjacent teeth are unrestored, it might remain preferable to use implants rather than prepare the unrestored teeth and live with esthetic compromise.
Slow orthodontic eruption before extraction is another option to consider when it is necessary to remove multiple adjacent teeth with periodontal disease.15 The eruption of a single tooth to be extracted does not alter the final papilla heights because they are dictated by the bone on the adjacent teeth. When multiple teeth are erupted before extraction, it is possible, but not always predictable, to move the interproximal bone coronally. However, it is critical to apprise the patient that a perfect esthetic result is unlikely, and that short papilla, long contacts, and more rectangular-looking final restorations could be expected (Figure 19, Figure 20, Figure 21, Figure 22, Figure 23 and Figure 24).
Teeth Are Missing
The next two presentations are the most difficult to manage esthetically because, in both cases, the teeth have already been removed. When this happens, the bony ridge tends to flatten rapidly unless something is done to alter the process. This means that in cases where the teeth have been missing for a significant period of time, the interproximal crest of bone is completely gone, and it is difficult and unpredictable to recreate it through vertical bone augmentation. Accordingly, when the teeth are missing before any treat-
ment, using adjacent implants invariably results in an inadequate papillary height. Using a connective graft and pontics, however, can create and maintain significantly more soft tissue above the interproximal bone than is possible with adjacent implants. The patient must be informed that the best esthetic result may involve pontics instead of implants. However, connective tissue grafting and a pontic next to implants can create an excellent result (Figure 25, Figure 26, Figure 27 and Figure 28).
Conclusion
The purpose of this article has been to evaluate the potential conditions that may present in patients who need or already have had multiple anterior tooth extractions, as well as to consider when the use of ovate pontics is warranted. The ultimate treatment decisions for individual patient management must occur on a case-by-case basis. It is critical to recognize in advance the various potential outcome possibilities that exist as a result of each patient’s presenting condition to make the most informed and realistic decisions about the best treatment options.
Acknowledgments
The author thanks Dr. Greggory Kinzer and Dr. Bobby Butler for Figure 5 through Figure 9; Dr. David Mathews, Dr. Vince Kokich, and Dr. Barret Rochefort for Figure 19 through Figure 24; and Dr. David Mathews and Dr. Roger Lawton for Figure 25 through Figure 28.
References
1. Choquet V, Hermans M, Adriaenssens P, et al. Clinical and radiographic evaluation of the papilla level adjacent to single-tooth dental implants. A retrospective study in the maxillary anterior region. J Periodontol. 2001;72(10):1364-1371.
2. Grunder U. Stability of the mucosal topography around single-tooth implants and adjacent teeth: 1-year results. Int J Periodontics Restorative Dent. 2000;20(1):11-17.
3. Kan JY, Rungcharassaeng K, Umezu K, et al. Dimensions of peri-implant mucosa: an evaluation of maxillary anterior single implants in humans. J Periodontol. 2003;74(4):557-562.
4. Tarnow DP, Magner AW, Fletcher P. The effect of the distance from the contact point to the crest of the bone on the presence or absence of the interproximal dental papilla. J Periodontol. 1992;63(12):995-996.
5. van der Velden U. Regeneration of the interdental soft tissues following denudation procedures. J Clin Periodontol. 1982;9(6):455-459.
6. Kois JC. Predictable single-tooth peri-implant esthetics: five diagnostic keys. Compend Contin Educ Dent. 2004;25(11):895-900.
7. Smukler H, Castellucci F, Capri D. The role of the implant housing in obtaining aesthetics: generation of peri-implant gingivae and papillae—Part 1. Pract Proced Aesthet Dent. 2003;15(2):141-149.
8. Salama H, Salama MA, Garber D, et al. The interproximal height of bone: a guidepost to predictable aesthetic strategies and soft tissue contours in anterior tooth replacement. Pract Periodontics Aesthet Dent. 1998;10(9):1131-1141.
9. Elian N, Jalbout ZN, Cho SC, et al. Realities and limitations in the management of the interdental papilla between implants: three case reports. Pract Proced Aesthet Dent. 2003;15(10):737-744.
10. Saadoun AP, Le Gall MG, Touati B. Current trends in implantology: part II—treatment planning, aesthetic considerations, and tissue regeneration. Pract Proced Aesthet Dent. 2004;16(10):707-714.
11. Hermann JS, Cochran DL, Nummikoski PV, et al. Crestal bone changes around titanium implants. A radiographic evaluation of unloaded nonsubmerged and submerged implants in the canine mandible. J Periodontol. 1997;68(11):1117-1130.
12. Hermann JS, Buser D, Schenk RK, et al. Crestal bone changes around titanium implants. A histometric evaluation of unloaded non-submerged and submerged implants in the canine mandible. J Periodontol. 2000;71(9):1412-1424.
13. Tarnow DP, Cho SC, Wallace SS. The effect of inter-implant distance on the height of inter-implant bone crest. J Periodontol. 2000;71(4):546-549.
14. Spear FM. Maintenance of the interdental papilla following anterior tooth removal. Pract Periodontics Aesthet Dent. 1999;
11(1):21-28.
15. Salama H, Salama M, Kelly J. The orthodontic-periodontal connection in implant site development. Pract Periodontics Aesthet Dent. 1996;8(9):923-932.
About the Author
Frank M. Spear, DDS, MSD
Founder and Director of the Seattle Institute for Advanced Dental Education
Affiliate Assistant Professor
University of Washington School of Dentistry
Private Practice
Seattle, Washington