You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
Throughout dental history, dentists have continually searched for the ideal restorative material. Dental ceramics commonly are used to serve this purpose because they are biocompatible and semitransparent in appearance; and they can create esthetic restorations, bear heavy loads, and have a thermal expansion coefficient suitable for dental structure. Currently, studies on porcelain have intensified, especially research on the durability, surface features, and esthetics of this restorative material.1,2
The Importance of a Smooth Surface
The surface of all dental restorative materials should be esthetic and smooth. A smooth surface is important in three terms: function, esthetics, and biologic compatibility. Rough surfaces can decrease the flexural strength of material.3 Opposite hard tissues can be abraded, and consequently, the restored teeth can become worn.4-6 Stain, plaque, and tartar can accumulate.5,7 As a result, the susceptibility to infection in oral soft tissues and caries increases.8,9 Because the free surface energy is lower at uneven surfaces than at smooth ones, microorganisms can easily adhere and colonize.10,11 Further, the esthetic quality of the restoration can decrease.12
With ceramic restorations, the glaze process helps prevent some of these problems. Plaque cannot accumulate on the glazed surface, and the brightness and surface features of the restoration can be retained long term.13 A smooth surface improves the flexural strength of the restoration and decreases abrasion against opposite teeth.14,15
Literature Studies
The literature clearly shows that grinding, polishing, and glazing increase a restoration’s flexural strength. Many studies found that mechanical polishing increases the surface resistance of a ceramic restoration more than the natural glaze and overglaze processes do.16-18 On the contrary, Sherill and O’Brien19 could not find any difference in flexural strength between ceramics that were mechanically polished and those that were glazed; however, Giordano et al14 found that overglazing, grinding, and polishing all significantly increased the flexural strength of ceramic restorations.
Methods to Generate a Smooth Surface
Glaze Process
Before final cementation, a restoration should have a completely smooth surface. This surface can be created only during the final glaze process in the dental laboratory. However, superficial defects can be covered with a surface polisher. The goal is to cycle the restoration through a porcelain furnace at a time and temperature schedule that achieves the proper surface quality, without causing any functional or esthetic damage.20-23
A lower temperature and longer time cycle should be the ceramist’s basic aim. In this way, the pyroplasticity of the crown is controlled to a level at which the surface will assume an enamel-like sheen but will not slump or flow at critical line angles. The ceramist must be aware that as the furnace temperature rises, the viscosity of dental glasses decreases. The ceramist must control this viscosity and use it to his or her advantage.23
A natural-appearing restoration surface can be created with two different glazing methods: overglaze (also called applied glaze) and natural glaze (also called self glaze).22,24 Overglaze is the addition of glass material that is vitrified at a low temperature and decreases the heat of fusion. Natural glaze keeps the surface of material at the temperature of its last firing without adding other materials.25
Overglaze technique: When external stains need to be applied or a labial margin needs to be created, the porcelain should not be exposed to high temperatures, ruling out a natural glazing. Overglazing should be used to prevent damage to the stains or labial margin. Overglaze is generated by exposing a low-temperature porcelain (generally) to a temperature that is 20°C to 60°C below the firing temperature.23,26
Natural glaze technique: A natural glaze refers to the process in which the restoration is fired to a temperature that is usually equal to or slightly higher than the original firing temperature. If the crown is to have a natural glaze, it will be fired after the stains are applied, according to the porcelain manufacturer’s instructions. The restoration should first be allowed to dry at the entrance of the furnace muffle until the stain medium has evaporated completely, leaving a dry, chalky surface. Then, the crown is inserted into the furnace slowly and fired to the manufacturer’s recommended glazing temperature for a short period, usually 1 to 2 minutes, until the outer surface of the porcelain develops the desired level of gloss. The porcelain surface of the restoration is exposed to temperatures high enough to permit the porcelain to fuse together and create a smooth, glossy outer “skin.” This process is performed at atmospheric pressure. The irregularities and superficial defects on the porcelain surface are closed while the surface melts slightly during firing, creating a smooth and glazed surface.24,27
Mechanical Polishing
Although dental porcelains almost meet the needs expected from a restorative material, they have an important disadvantage. These materials may cause opposite dental structures to be extremely abraded. Most damage happens with contact of uneven surfaces under the occlusive forces. Besides occlusal regulations, acidulated phosphate fluoride applications, carbonated beverages, or air-powder abrasion processes can create unevenness after a restoration is placed. Periodic repair of uneven porcelain surfaces can decrease the abrasion on teeth, reduce the risk of porcelain fracture, and provide the continuity of biologic and esthetic criteria by avoiding accumulation of tartar.28-31
When a porcelain surface loses its luster, it needs to be repolished. It can be either reglazed or polished with various polishing instruments and pastes. The restoration is polished in the patient’s mouth or reglazed in the dental laboratory. When a restoration is reglazed, chairtime for the patient is minimal. However, because reglazing is performed at the dental laboratory, it requires multiple office visits. Ceramic restoration in a furnace at high temperatures may cause destruction because of trapped moisture from the saturation in the oral environment; therefore, in-laboratory reglazing is typically considered not the best option. After the reglazing procedure, the laboratory technician repolishes the surface extraorally, which allows greater control of the polish.32,33 For this reason, literature studies concentrate on the effects of diamond drills, flexible discs, silicone polishers, and diamond polishing pastes.34,35 Although intaroral polishing is rarely performed in the United States, studies have found that the preferred techniques for repolishing are: 1) smoothing the contours with flexible diamond discs, diamond burs, polymer stones, or green stones (silicon carbide); 2) finishing with white stones or rubber discs and conical-shaped rubber tips; and 3) polishing with diamond pastes and felt, conical-shaped or thin rubber discs, or a brush.36,37
Many studies focused on determining the best method of creating a smooth surface on ceramic restorations. A literature review revealed that glazing or mechanical polishing methods are performed to re-create a smooth surface. Generally, stones or diamond drills are used to correct the ceramic before an overglaze or natural glaze is applied. The authors found that most studies on uneven surface texture are oriented toward determining the efficacy or deficiency of mechanical polishing compared with natural glaze or overglaze processes.
Most of these studies used abraders consecutively (diamond bur, rubber disc, diamond paste) or a sequential set of polishers from an available polishing kit. Some studies of the consecutive polishing method used diamond paste in the final phase.12,15,38-40 Other studies used available kits without diamond paste.40-42 Raimondo and colleagues43 preferred the All Ceramic Finishing and Polishing Kit (Shofu Dental Corp, www.shofu.com), while Hulterström and Bergman,44 as well as Shearer and colleagues,45 preferred the Sof-Lex™ Finishing and Polishing System (3M ESPE, www.3MESPE.com). Both of these kits contain rubber discs in descending grits—rough, intermediate, thin, and super thin.46
The Sof-Lex discs are coated with aluminum oxide. According to the manufacturer, the operator must use all four grits to achieve surface smoothness, ending with super fine. Further, a study by the manufacturer found that when using the Sof-Lex Finishing and Polishing System, the addition of diamond paste does not increase surface smoothness in ceramic restorations.36
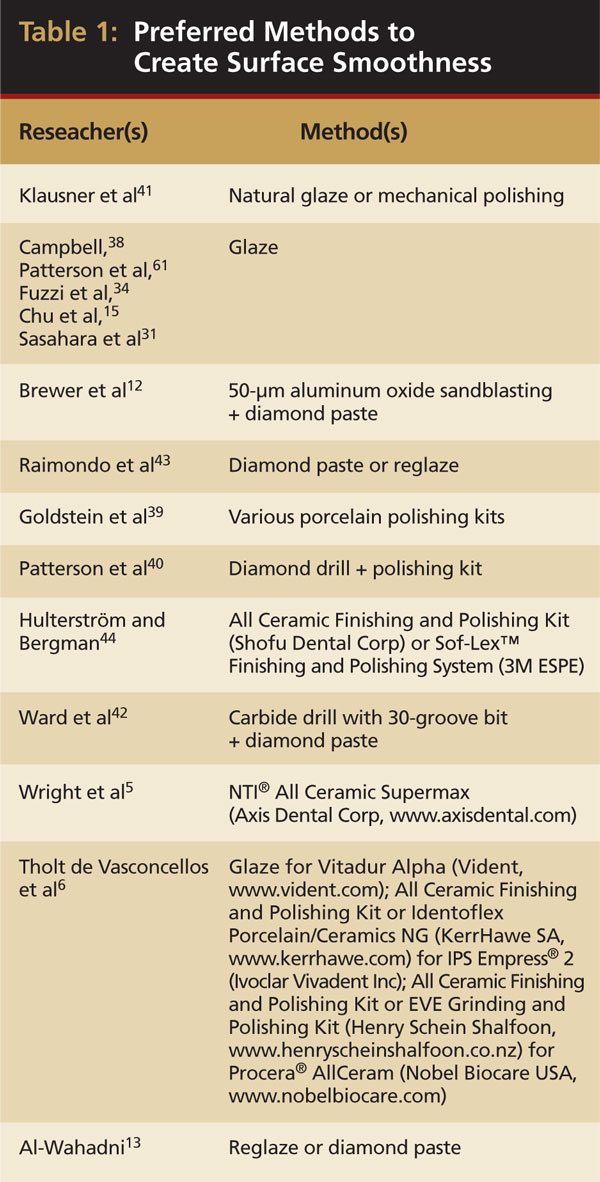
Table 1 summarizes the findings of published studies that compared glazing and mechanical polishing. On review, the authors found that the study results depended on which ceramic and polishing method was used. For example, Patterson and colleagues40 declared that if diamond burs are used before a polishing kit, the resulting ceramic surface is smooth, but not as smooth as when glaze is applied.
Polishing efficacy also depends on each material’s structure. For example, Sasahara and colleagues31 found the degree of surface smoothness achieved was based on the leucite content of the porcelain. Further, they noted that to find the appropriate polishing method for each ceramic can be difficult because of varying microstructures. The researchers emphasized that using a ceramic with low leucite content and applying a diamond paste during polishing can increase surface smoothness. To further this point, Al-Wahadni13 found that a high crystal content in a ceramic material can lead to an uneven surface when polished.
Repeated Firings
Although dental porcelains and the preparation techniques have evolved, achieving an esthetic match with the existing dentition can be difficult and require careful planning. Because gold is expensive, there is interest in base metal alloys as the supporting structure of porcelain-fused-to-metal ceramic restorations. Before being placed on the market, these alloys were studied in both laboratory and clinical settings. Besides various compatibility tests (connection, thermal, contour clarity), the studies examined the effect of repeated firings on color, fluorescence, microstructure, and brightness of the fused porcelains.47-51
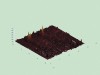
The solvents were added by manufacturers to decrease the heat of fusion in porcelains. These solvents have a high rate of fluidity, which helps form a glazed surface. However, the thickness of this glaze layer can decrease from repeated firings and intraoral abrasion. The surface is softened, and the glaze layer is removed by repeated firings, decreasing the surface roughness (Figure 1A through Figure 2E). The mean matrix of porcelain structure, being highly fluid, moves toward the surface of the porcelain and helps form a natural glazed surface. The necessary amount of matrix required to form a natural glazed surface decreases after repeated firings.49
As the number of firings increases, the dimensions of the pores in a porcelain’s structure decrease, creating a vitreous structure. This decrease in the dimensions of the pores causes the porcelain’s rigidity to increase and its flexibility to decrease.52 Repeated firings also cause porcelain’s color pigments to burn and a mass of porcelain to accumulate, creating devitrification. The authors conclude that, based on available data, repeated firings of porcelain restorations should be minimized.49,52
Studies on the effects of repeated firings on surface smoothness are limited. Barghi49 researched the effects of repeated firings on color and glaze and found that after nine firings, a natural glaze layer appears on the surface and the choice of metal alloy did not affect the color or glaze. Mackert and Williams53 researched the effects of repeated firings on the formation of microfractures in the ceramic. They concluded that repeated firings affected the density of microfracture after one, three, seven, and 15 firings but that this finding was not clinically significant. Özkan and Öztas54 researched the effects of repeated firings on leucite crystals in dental ceramics. They determined that after repeated firings, the porcelain structure and the diffraction pattern of leucite crystals exhibited minimal change, which was not clinically significant. Isgrò and colleagues55 researched the effects of repeated firings on thermal distortion in one glass ceramic core, four commercially available veneering porcelains, and two experimental veneering porcelain materials. Measurements on the phase of wash, 1st dentine, 2nd dentine, 1st glaze, and 2nd glaze, were made by using the examples of different veneer ceramics; consequently, the researchers concluded that the thermal expansion coefficient is associated with chemical structure. It was found that when compared with other ceramic compositions, those consisting of glass and aluminum display a more stabile and resistive manner during repeated firings.
Methods to Assess Surface Roughness
Visual assessment, scanning electron microscopy (SEM), profilometry, laser specular reflectance, or atomic force microscopy (AFM) devices can be used for investigating the surface of dental materials.56
Profilometry devices commonly are used for assessing the roughness of a material’s surface. A diamond-scanning probe on the device examines the sample’s surface, and the findings of surface roughness are calculated digitally and recorded.57 Many parameters can be assessed using profilometry devices, with the most common being average roughness deviation (Ra) and root-mean-square (rms) roughness deviation (Rq).58 AFM is used for the studies of abrasion, binding, cleansing, corrosion, acidification, friction, lubrication, and coating. AFM systems use a topographic surface view at the nanometer level to measure the forces between molecules (nN, pN).57,59,60
A review of the literature revealed that usually SEM and profilometry31,34,39,41,42,61 or rarely SEM and visual assessment43 or AFM and profilometry6 are used together. There are also studies that used a single method to analyze the surface smoothness of dental ceramics, for example, SEM,38 visual assessment,12 AFM,62 laser specular reflectance system,45 or profilometry.13,63
Investigating a ceramic’s surface with AFM provides a 3-dimensional (3D) view and allows high-resolution topographic imaging of sample surfaces. Compared with profilometry and visual assessment, AFM provides greater detail. AFM gives the Ra values of the measured samples. Various details can be observed including densely located elevations or valleys; tiny, small, and spiny juts; smooth and flat parts; cracks, breaches, craters, or holes; wide-angled and round elevations and valleys; deteriorated surface images; asymmetric or parallel areas; and shiny, smooth surfaces.6,62,64 Although AFM can be performed directly on the material’s surface (without a coating), its 3D topographic view and numerical parameters of surface smoothness are difficult to repeat because the scanning field is smaller than in other methods.65,66
Conclusion
With today’s ceramic materials, older restorations whose surfaces have roughened can be resmoothed with finishing and polishing products.13 Using various intraoral and extraoral porcelain polishing kits, smoothness levels equal or better than those attained through glazing procedures can be obtained.31
Rough surfaces lead to many problems, including lower flexural strength, abrasion on opposite hard tissues, staining of restoration surfaces, accumulation of plaque and tartar, infection of oral soft tissues, and caries formation. When a porcelain surface loses its luster, it needs to be repolished. It can be either reglazed or polished with various polishing instruments and pastes. Ceramic restoration in a furnace at high temperatures may cause destruction because of trapped moisture from the saturation in the oral environment. For this reason, literature studies concentrate on the effects of diamond drills, flexible discs, silicone polishers, and diamond polishing pastes.
Visual assessment, SEM, profilometry, laser specular reflectance, or AFM devices can be used for investigating the surface of dental materials. Examining a ceramic’s surface with AFM provides a 3D view and high-resolution topographic imaging of sample surfaces compared with profilometry and visual assessment. AFM gives the value of mean surface roughness, and various details may be observed, including densely located elevations or valleys; tiny, small, and spiny juts; smooth and flat parts; cracks, breaches, craters or holes; wide-angled and round elevations and valleys; deteriorated surface images; asymmetric or parallel areas; and shiny, smooth surfaces.
References
1. Jacobi R, Shillinburg HT Jr, Duncanson MG. A comparison of the abrasiveness of six ceramic surfaces and gold. J Prosthet Dent. 1991;66(3):303-309.
2. Rosenblum MA, Schulman A. A review of all-ceramic restorations. J Am Dent Assoc. 1997;128(3):297-307.
3. Bessing C, Wiktorsson. A comparison of two different methods of polishing porcelain. Scand J Dent Res. 1983;91(6):482-487.
4. al-Hiyasat AS, Saunders WP, Sharkey SW, et al. The abrasive effect of glazed, unglazed, and polished porcelain on the wear of human enamel, and the influence of carbonated soft drinks on the rate of wear. Int J Prosthodont. 1997;10(3):269-282.
5. Wright MD, Masri R, Driscoll CF, et al. Comparison of three systems for the polishing of an ultra-low fusing dental porcelain. J Prosthet Dent. 2004;92(5):486-490.
6. Tholt de Vasconcellos B, Miranda-Júnior WG, Prioli R, et al. Surface roughness in ceramics with different finishing techniques using atomic force microscope and profilometer. Oper Dent. 2006;31(4):442-449.
7. Clayton JA, Green E. Roughness of pontic materials and dental plaque. J Prosthet Dent. 1970;23(4):407-411.
8. Kawai K, Urano M, Ebisu S. Effect of surface roughness of porcelain on adhesion of bacteria and their synthesizing glucans. J Prosthet Dent. 2000;83(6):664-667.
9. Martinez-Gomis J, Bizar J, Anglada JM, et al. Comparative evaluation of four finishing systems on one ceramic surface. Int J Prosthodont. 2003;16(1):74-77.
10. Bollen CML, Lambrechts P, Quirynen M. Comparison of surface roughness of oral hard materials to the threshold surface roughness for bacterial plaque retention: a review of the literature. Dent Mater. 1997;13(4):258-269.
11. de Silva MFA, Davies RM, Stewart B, et al. Effect of whitening gels on the surface roughness of restorative materials in situ. Dent Mater. 2006;22(10):919-924.
12. Brewer JD, Garlapo DA, Chipps EA, et al. Clinical discrimination between autoglazed and polished porcelain surfaces. J Prosthet Dent. 1990;64(6):631-634.
13. Al-Wahadni A. An in vitro investigation into the surface roughness of 2 glazed, unglazed and refinished ceramic materials. Quintessence Int. 2006;37(4):311-317.
14. Giordano RA, Cima M, Pober R. Effects of surface finish on the flexural strength of feldspathic and aluminous dental ceramics. Int J Prosthodont. 1995;8(4):311-319.
15. Chu FCS, Frankel N, Smales RJ. Surface roughness and flexural strength of self-glazed, polished, and reglazed in-ceram/vitadur alpha porcelain laminates. Int J Prosthodont. 2000;13(1):66-71.
16. Williamson RT, Kovarik RE, Mitchell RJ. Effects of grinding, polishing, and overglazing on the flexure strenght of a high-leucite feldspathic porcelain. Int J Prosthodont. 1996;9(1):30-37.
17. Rosenstiel SF, Baiker MA, Johnston WM. A comparison of glazed and polished dental porcelain. Int J Prosthodont. 1989;2(6):524-529.
18. Giordano RA 2nd, Campbell S, Pober R. Flexural strength of feldspathic porcelain treated with ion exchange, overglaze, and polishing. J Prosthet Dent. 1994;71(5):468-472.
19. Sherill CA, O’Brien WJ. Transverse strength of aluminous and feldspathic porcelain. J Dent Res. 1974;53(3):683-690.
20. Wiley MG. Effects of porcelain on occluding surfaces of restored teeth. J Prosthet Dent. 1989;61(2):133-137.
21. Zaimoǧlu A, Can G, Ersoy AE, et al. Diş Hekimliǧinde Maddeler Bilgisi. Ankara: Ankara Üniversitesi Yayınları; 1993:chapter 16.
22. Craig RG, Powers JM, eds. Restorative Dental Materials. 11th ed. St. Louis, MO: Mosby Company; 2002.
23. McLean JW. The Science and Art of Dental Ceramics. Volume I: The Nature of Dental Ceramics and Their Clinical Use. Chicago, IL: Quintessence Publishing Co; 1979:Monograph 1.
24. Naylor WP, Kessler J, King A. Introduction to Metal Ceramic Technology. Chicago, IL: Quintessence Publishing Co; 1992:157-161.
25. Sarac D, Sarac S, Yüzba¸sıo˘glu E, et al. The effects of porcelain systems on the color and surface texture of feldspathic porcelain. J Prosthet Dent. 2006;96(20):122-128.
26. Tamura K. Essentials of Dental Technology. Chicago: Quintessence Publishing Co; 1987:390-392.
27. Cook PA, Griswold WH, Post AC. The effect of superficial colorant and glaze on the surface texture of vacuum fired porcelain. J Prosthet Dent. 1984;51(4):476-484.
28. Eliades GC, Tzoutzas JG, Vougiouklakis GJ. Surface alterations on dental restorative materials subjected to an air-powder abrasive instrument. J Prosthet Dent. 1991;65(1):27-33.
29. Ma T, Johnson GH, Gordon GE. Effects of chemical disinfectants on surface characteristics and color of three fixed prosthodontic crown materials. J Prosthet Dent. 1999;82(5):600-607.
30. Alkhiary YM, Morgano SM, Giordano RA. Effects of acid hydrolysis and mechanical polishing on surface residual stresses of low-fusing dental ceramics. J Prosthet Dent. 2003;90(2):133-142.
31. Sasahara RMC, Riberio FC, Cesar PF, et al. Influence of the finishing technique on surface roughness of dental porcelains with different microstructures. Oper Dent. 2006;31(5):557-583.
32. O’Brien WJ, ed. Dental Materials and Their Selection. 3rd ed. Chicago, IL: Quintessence Publishing Co; 2002: chapter 10.
33. Kelly JR. Dental ceramics: current thinking and trends. Dent Clin North Am. 2004;48(2):513-530.
34. Fuzzi M, Zaccheroni Z, Vallania G. Scanning electron microscopy and profilometer evaluation of glazed and polished dental porcelain. Int J Prosthodont. 1996;9(5):452-458.
35. Magne P, Belser U. Bonded Porcelain Restorations in the Anterior Dentition: A Biomimetic Approach. Chicago, IL: Quintessence Publishing Co; 2002: chapter 7.
36. Jefferies SR. The art and science of abrasive finishing and polishing in restorative dentistry. Dent Clin North Am. 1998;42(4):613-627.
37. Al-Wahadni A, Martin DM. An in vitro investigation into the wear effects of glazed, unglazed and refinished dental porcelain on an opposing material. J Oral Rehabil. 1999;26(6):538-546.
38. Campbell SD. Evaluation of surface roughness and polishing techniques for new ceramic materials. J Prosthet Dent. 1989;61(5):563-568.
39. Goldstein GR, Barnhard BR, Penugonda B. Profilometer, SEM, and visual assessment of porcelain polishing methods. J Prosthet Dent. 1991;65(5):627-634.
40. Patterson CJW, McLundie AC, Stirrups DR, et al. Refinishing of porcelain by using a refinishing kit. J Prosthet Dent. 1991;65(3):383-388.
41. Klausner LH, Cartwright CB, Charbeneau GT. Polished versus autoglazed porcelain surfaces. J Prosthet Dent. 1989;47(2):157-162.
42. Ward MT, Tate WH, Powers JM. Surface roughness of opalescent porcelains after polishing. Oper Dent. 1995;20(3):106-110.
43. Raimondo RL, Richardson JT, Wiedner B. Polished versus autoglazed dental porcelain. J Prosthet Dent. 1990;64(5):553-557.
44. Hulterström AK, Bergman M. Polishing systems for dental ceramics. Acta Odontol Scand. 1993;51(4):229-234.
45. Shearer AC, Kusy RP, Whitley JQ, et al. Finishing of MGC Dicor material. Int J Prosthodont. 1994;7(2):167-173.
46. Al-Wahadni A, Martin DM. Glazing and finishing dental porcelain: a literature review. J Can Dent Assoc. 1998;64(8):580-583.
47. Jorgenson MW, Goodkind RJ. Spectrophotometric study of five porcelain shades relative to the dimensions of color, porcelain thickness, and repeated firings. J Prosthet Dent. 1979;42(1):96-105.
48. Buchanan WT, Svare CW, Turner KA. The effect of repeated firings and strength on marginal distortion in two ceramometal systems. J Prosthet Dent. 1981;45(5):502-506.
49. Barghi N. Color and glaze: effects of repeated firings. J Prosthet Dent. 1982;47(4):393-395.
50. Dederich DN, Svare CW, Peterson LC, et al. The effect of repeated firings on the margins of nonprecious ceramometals. J Prosthet Dent. 1984;51(5):628-630.
51. Ecker GA, Moser JB, Wozniak WT, et al. Effect of repeated firing on fluorescence of porcelain-fused-to-metal porcelains. J Prosthet Dent. 1985;54(2):207-214.
52. Öztaş DD, Kaplan R, Atakol O, et al. The effect of glaze thickness of the microstructure of low fusing dental porcelain. Abstract presented at: 6th Congress of the Balkan Stomatological Society; May 3-6, 2001; Bucharest, Romania.
53. Mackert JR Jr, Williams AL. Microcracks in dental porcelain and their behavior during multiple firing. J Dent Res. 1996;75(7):1484-1490.
54. Özkan P, Özta¸s DD. Dental porselenlerde tekrarlanan fırınlamaların lösit kristalleri üzerinde etkisi. T Klin Dis Hek Bil Derg. 2000;6:101-107.
55. Isgrò G, Kleverlaan C J, Wang H, et al. Thermal dimensional behavior of dental ceramics. Biomaterials. 2004;25(12):2447-2453.
56. Anusavice KJ. Phillips’ Science of Dental Materials. 11th ed. St. Louis, MO: Saunders; 2003: chapters 13, 21.
57. Bourauel C, Fries T, Drescher D, et al. Surface roughness of orthodontic wires via atomic force microscopy, laser specular reflectance and profilometry. Eur J Orthod. 1998;20(1):79-92.
58. Whitehead SA, Shearer AC, Watts DC, et al. Comparison of methods for measuring surface roughness of ceramic. J Oral Rehabil. 1995;22(6):421-427.
59. Aydın A. Investigation of Fractal Dimension on Atomic Force Microscopic Images [thesis]. Ankara, Turkey: Dept of Physics, Middle East Technical University; 2001.
60. Doǧan M. Kimyada nanoteknoloji devri. Kimya Teknol Derg. 2005;57:20-24.
61. Patterson CJW, McLundie AC, Stirrups DR, et al. Efficacy of a porcelain refinishing system in restoring surface finish after grinding with fine and extra-fine diamond burs. J Prosthet Dent. 1992;68(3):402-406.
62. Demirel F, Yüksel G, Muhtaroǧulları M, et al. Effect of topical fluorides and citric acid on heat-pressed all-ceramic material. Int J Periodontics Restorative Dent. 2005;25(3):277-281.
63. Camacho GB, Vinha D, Panzeri H, et al. Surface roughness of a dental ceramic after polishing with different vehicles and diamond pastes. Braz Dent J. 2006;17(3):191-194.
64. Folwaczny M, Mehl A, Haffner C, et al. Polishing and coating of dental ceramic materials with 308 nm XeCl excimer laser radiation. Dent Mater. 1998;14(3):186-193.
65. Silikas N, Watts DC, England KE, et al. Surface fine structure of treated dentine investigated with tapping mode atomic force microscopy (TMAFM). J Dent. 1999;27(2):137-144.
66. Teixeria ECN, Thompson JI, Piascik JR, et al. In vitro toothbrush-dentifrice abrasion of two restorative composites. J Esthet Restor Dent. 2005;17(3):172-182.
About the Authors
Kerem Yılmaz, DDS, Prosthodontist, Department of Prosthodontics, Faculty of Dentistry, University of Ankara, Turkey
Pelin Özkan, DDS, Associate Professor, Department of Prosthodontics, Faculty of Dentistry, University of Ankara, Turkey