You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
The predictability and success of an implant-supported restoration depends on the volume and quality of bone available for the implant fixture. In the maxillary arch, loss of alveolar bone height severely compromises the bone’s retention capacity. Implant placement in the posterior maxilla often is complicated by reduced bone quality and limited bone height. Therefore, placement of a dental implant may be difficult because of severe alveolar bone resorption or pneumatization of the sinuses. In these cases, augmentation of the maxillary sinus to increase bone volume is a prerequisite for successful implant placement in the posterior maxilla.
MAXILLARY SINUS ANATOMY
The nasal cavity is surrounded by four paranasal sinuses that are located in the maxillary, frontal, sphenoid, and ethmoid bones. The maxillary sinuses are the largest, located lateral to the nasal cavities.1 They are pyramidal shaped with the base at the lateral nasal wall and the tip at the zygomatic bone.2 This tip is connected to the nasal cavity by the ostium which opens into the middle nasal meatus under the overlapping middle nasal turbinate. The sinus membrane consists of ciliated pseudostratified columnar epithelium and its main function is to transport the fluids that the sinus drains.
The maxillary bone is spongy and finely trabecular; however, occasionally a bony septum can be found separating the sinus into different cavities. These bony septa are located primarily in the middle portion of the maxillary sinus (41%), but they can be located in the most mesial (24%) and distal (35%) extensions of the sinus.3,4 When bony septa are present, sinus augmentation is more challenging for the clinician because the septum is associated with a higher possibility of membrane perforations.2 The average dimensions are 38 mm in height, 33 mm in width, and 38 mm in length, and the sinus pneumatizes with loss of teeth.2 The volume of the maxillary sinus increases with age and tooth loss, ranging from 4.5 cm3 to 35.2 cm3. Size and shape varies between individuals. The blood supply to the maxilla emanates from three arteries: the superior labial, the anterior ethmoidal and, primarily, the internal maxillary. The sinus floor receives some of the blood supply from the greater palatine and lesser palatine vessels as well as the incisal artery, which is a terminal branch of the sphenopalatine artery. Venous drainage is via the sphenopalatine medially and pterygoid plexus for all other aspects, while V2 of the trigeminal nerve (maxillary branch) supplies sensory intervention.
The main functions of the maxillary sinus are to (1) give resonance to the voice; (2) lighten the weight of the skull; (3) warm and moisten inspired air; (4) secrete and store mucus; (5) characterize contour of the face; and (6) preserve warmth from the nasal fossa.5 Compared with other sinuses, the maxillary sinus has fewer blood vessels, osteoblasts, and elastic fibers. The fewer osteoblasts may account for continued pneumatization, and the fewer elastic fibers may make elevation easier.2 The continuous enlargement of the maxillary sinus throughout life may limit the quantity of residual crestal bone remaining for implant placement.
HISTORY OF MAXILLARY SINUS AUGMENTATION
In the early 1960s,
INDICATIONS AND CONTRAINDICATIONS FOR SINUS LIFT/IMPLANT PLACEMENT
Teeth maintain the height of the maxillary sinus; after tooth loss, the sinus expands or pneumatizes, reducing the quantity of available bone. Maxillary molars are the most common teeth to be lost.8,9 The main reasons for tooth loss are dental caries and periodontal disease; other reasons can be root fracture or endodontic complications. Thus, replacement of missing teeth in the posterior maxilla may require a sinus lift procedure to restore the lost bone. The sinus lift procedure is somehow invasive, and has its indications and contraindications. Indications include healthy or medically well-controlled patients. There should be no pathology present within the sinus. For the purpose of implant placement and restoration, the need for a sinus graft procedure also is assessed, based on the amount of residual bone following sinus pneumatization. Radiographic evaluation with use of plain films (
Contraindications may include a medical condition that is not well controlled (ie, uncontrolled diabetes mellitus, hypertension, cardiovascular disease, immune disorders, etc), heavy smokers (³ 20 cig/day), pathology or severe congestion within the sinus where an otolaryngologic intervention is necessary, and deformity or radiation therapy to the sinus.12 Such conditions will predispose patients to postsurgical complications, such as graft mass infection, loss of the augmented bone, and oroantral fistula. Therefore, contraindications for sinus augmentation likely will include one or several of the previously mentioned risk factors.
TREATMENT PLANNING
Clinical situations requiring sinus grafting vary from a single missing tooth to reconstruction of the completely edentulous posterior segment. To effectively analyze and determine surgical requirements, the clinician must:
1. determine the medical status of the patient (certain medical conditions will prevent the application of such procedures).
2. establish a comprehensive treatment plan with the desired outcome envisioned before the surgery.
3. examine the site radiographically via a panoramic film and/or computed tomography scan. This will determine the required volume of bone along with detecting pathologies and abnormalities directly or indirectly affecting the maxillary sinus.
4. determine the location, orientation, and number of implants through correctly mounted diagnostic study models, along with an anatomically correct waxup, ultimately leading to the fabrication of a surgical stent.13
In regard to remaining bone volume, Fugazzotto evaluated the relationship between preoperative residual alveolar bone crestal to the floor of the sinus and the width of the ridge to determine the type of augmentation therapy required.14 Thus, depending on the amount of the residual bone height, different techniques can be performed, from a lateral window sinus lift to an osteotome sinus technique.
SURGICAL TECHNIQUES
A variety of techniques exist to elevate the sinus floor in preparation for implant placement. This article will concentrate on the two most commonly used techniques: Caldwell-Luc (the lateral window sinus bone augmentation) and the osteotome assisted internal sinus floor elevation. Several variations exist, such as the hydraulic sinus condensing technique, the trephine osteotomy, and others.
Lateral Window Technique
After the patient receives profound local anesthesia, crestal and vertical incisions are made and a full thickness flap is elevated toward the buccal. A window is outlined on the lateral border of the sinus (buccal alveolar ridge in posterior maxilla) with a diamond bur in a low-speed handpiece or piezoelectric surgery unit until a bluish hue is observed around the outlined window. The bony window is rotated horizontally with the sinus membrane and pushed inwards, becoming part of the elevated sinus. A curved elevator is inserted along the inferior border of the window to separate the membrane from the bone, and elevation is continued anteriorly, posteriorly, superiorly, and medially until complete elevation is established. The clinician must ensure that the sharp end of the elevator remains in contact with bone and the blunt end against the sinus membrane during elevation.15
The elevated membrane leaves an empty space in the lower third of the sinus that will be augmented with the bone graft. Then, a collagen membrane is used to cover the window, and the flaps are sutured passively to obtain primary closure. A healing period of approximately 6 months is recommended for initial bone maturation (Figure 1A through Figure 1I).
PIEZOELECTRIC SURGERY
The lateral window and osteotome techniques have been used frequently for sinus augmentation in the past few decades. Sinus membrane perforations have been associated with these two conventional treatments and, therefore, alternative approaches have been explored recently. The use of piezoelectric surgery as an alternative technique has been shown to have favorable results with fewer complications, such as sinus perforations.16,17 Piezoelectric surgery units use low-frequency ultrasonic vibrations that scatter upon contact with soft tissue and, thus, do not perforate the thin sinus membrane (Figure 2A). These units offer different surgical tips for bone and soft-tissue manipulation. Depending on bone thickness, a tip is chosen and used to outline the lateral window. Then, membrane elevation is continued with a conventional curved curette for the first 2 mm around the created bony window. Finally, piezoelectric surgical elevation tips are used for membrane elevation.1,18 The bone graft is introduced into the created space after sinus elevation (Figure 2B and Figure 2C), and the procedure is completed similarly to the lateral window technique.
SINUS AUGMENTATION COMBINED WITH GUIDED BONE REGENERATION
Lateral ridge augmentation often is performed in combination with sinus floor elevation, especially when the patient has been edentulous for a long duration. The application of a replacement bone graft well beyond the buccal aspect of the ridge will result in a wider ridge, thus accommodating the desired implant diameter. Autologous and/or particulate allograft can be used to achieve the desired augmentation. The ridge expansion technique is also a predictable option in ridges of ³ 3 mm in width.
Using either rotary burs or the appropriate piezoelectric surgical tip, a crestal osteotomy is performed along the length of the ridge, joined with two vertical bony cuts (Figure 3A). Ridge splitters, expanders, or chisels are inserted through the crestal cut in an attempt to expand gently and mobilize laterally the buccal bone plate. Then, the bone graft is applied internally, with or without immediate implant placement (Figure 3B through Figure 3D).
Internal Osteotome Technique
In an attempt to augment the atrophic maxillary sinus in anticipation of implant placement in a less invasive manner, Summers proposed the osteotome technique.7 This approach obviates the need for the preparation of a bony window in the lateral aspect of the alveolus, and its subsequent rotation to displace the maxillary sinus. Rather “an internal sinus lift” is performed through the use of sequentially sized osteotomes to implode residual alveolar bone crestal to the floor of the sinus, with or without simultaneous bone grafting. This technique can be performed in conjunction with simultaneous implant placement or to prepare a site for future implant placement. Although Summers did not mention the amount of residual crestal bone required, most studies have found a minimum of 6 mm of remaining bone between the crest and sinus floor is needed (Figure 4A).19,20
Summers’ osteotomes root analog instrument set consists of four calibrated instruments, with each consecutive osteotome increasing in diameter. The tips are concave and blunt, and are used to widen the osteotomy site. The twist drill is stopped 1 mm short of sinus floor and consecutive osteotomes advance the bone graft through the prepared site (Figure 4B and Figure 4C). Then, the hydraulic pressure of graft material raises the floor of the sinus, on average 4 mm20(Figure 4D and Figure 4E).
TYPES OF BONE GRAFT AND MEMBRANE MATERIALS
Multiple grafting materials have been used to augment the maxillary sinus, such as particulate bone grafts and block grafts from various sources. Particulate bone grafts have been reported to have a higher survival rate than block grafts.21 In general, bone grafting materials possess osteogenic (autograft), osteoinductive (autograft/allograft), or osteoconductive (xenograft/alloplast) properties. In regard to the type of particulate graft used, Cammack nd colleagues found no significant difference in the percentage of new bone induced by either freeze-dried bone allograft (FDBA) or demineralized freeze-dried bone allograft (DFDBA), regardless of the site augmented. In sinus augmentation, regeneration of ~42% new bone area occurred with no statistical difference between them.22 Therefore, the choice of bone graft is one of practitioner preference, not material performance.
The use of a barrier membrane over the lateral window has been shown to improve the success rate of implant survival in the grafted sinus.21 Moreover, the understanding of how a barrier creates space for selective cell repopulation gave rise to the concept of epithelial exclusion to restore lost periodontal tissue as well as guided bone regeneration. This is because of the variability in the types of periodontal tissues repopulating the area during healing. Melcher, in 1976, suggested that there are four different cell types dictating the type of periodontal healing that will occur.
These cells originate from the epithelial gingival tissue, the lamina propria of connective tissue, the bone, and the periodontal ligament.23 Thus, with the use of a membrane, cells derived from bone will have the potential to regenerate the lost bone volume within the sinus in the posterior maxilla. The most commonly placed membranes are resorbable (collagen membranes) rather than nonresorbable (expanded polytetrafluoroethelyne [e-PTFE]).
MANAGEMENT OF SINUS SEPTA
The incidence of sinus septum is 24% to 41%, with high variability in size and location; identification of the septum before the surgical sinus lift will reduce the possibility of complications.3,4 The location of the septum will dictate the size and design of the lateral wall osteotomy. The septum is isolated through careful lateral window osteotomy, defining two compartments mesial and distal to the septum. Figures 5A through Figure 5E illustrate proper management of the septum.
MEDICATIONS
Sinus elevation is considered an invasive procedure and, therefore, pre- and postoperative medications are indicated. Antibiotics are recommended to reduce the chance of infection (10%), and they usually are used preoperatively.24,25 The primary antibiotics prescribed include amoxicillin 500 mg, q 8 hrs, for 10 days, azithromycin 250 mg, q 12 hrs initially and once per day thereafter for 10 days, and clindamycin 150 mg, q 6 hrs, for 10 days. The use of antibiotics preoperatively within 24 hours is more effective than postoperatively for implant survival.26 Preoperative anti-inflammatory medications, such as nonsteriodal antiinflammatory drugs and corticosteroids, also are indicated. Common anti-inflammatory medications include ibuprofen 800 mg, q 8 hrs, for 5 days and Methylprednisolone dose pack in a tapering dose.27 Decongestants and antihistamines also may be prescribed for 14 to 21 days, once per day, beginning a few days before surgery and continued for 10 to 14 days after. Finally, chlorhexidine rinse, 0.12%, is prescribed as an antimicrobial and antigingivitis agent to reduce bacterial plaque accumulation in the surgical area postoperatively.28
POSTOPERATIVE INSTRUCTIONS
Patients should be strongly cautioned that they need to comply with all instructions and medications as prescribed by the clinician. Ice packs should be applied to the surgical area to minimize the chances of postoperative swelling. Patients should not apply any type of negative pressure, such as blowing their nose, any type of smoking, or using a straw, which can interfere with blood clot and wound closure. In addition, patients will need to be placed on a soft diet and instructed to avoid chewing on the surgical area to minimize unnecessary disturbances to the area. Plaque removal is necessary, accomplished by rinsing with chlorhexidine as well as swabbing the rinse gently on the surgical area. Finally, if no complications arise within the first few days, patients should be seen for postoperative evaluation at 1-, 3-, and 4-week intervals.29
PREDICTABILITY AND SUCCESS RATE FOR IMPLANTS IN AUGMENTED SINUSES
Regardless of the technique used to augment the sinus and place an implant, meticulous surgical technique and sufficient clinical experience are essential for a predictable outcome. In regard to the lateral window sinus lift, Wallace and Froum, in 2003, conducted a systematic review and found that it is advantageous to use particulate graft with roughened surface implants and cover the lateral window with a membrane to enhance implant survival and obtain more predictable outcomes.21 Membrane coverage of the lateral window showed a survival rate of 93.6% vs 88.7% when a membrane was not used. The use of particulate bone grafts had 92.3% survival rate vs 83.3% using block grafts. Rough-surfaced implants had 94.6% survival rate vs 90% machine-surfaced implants.21
Emmerich and Stappert, in 2005, conducted a systematic review and meta-analysis that included eight articles out of 44 potential publications that examined implant survival using the osteotome technique.30 The results were evaluated at 24 and 36 months, and indicated a survival and success rate of 95.7% and 96.0% respectively. The researchers concluded that short-term (< 3 yrs) clinical success/survival of implants placed using the osteotome technique is similar to that of implants placed in a partially edentulous maxilla.
POSTOPERATIVE COMPLICATIONS
As with any surgical procedure, complications may occur during or after surgery. Perforation of the sinus membrane is one of the main complications associated with a maxillary sinus lift. The presence of a septum (bony protuberance into the sinus) may increase the likelihood of perforations.
Vlassis and Fugazzotto suggested five different classes associated with lateral window sinus lift according to location and extent of perforation.32 When the perforation can be isolated, depending on the extent and location, repair can be performed by folding the sinus membrane over itself and placing a collagen membrane. If the perforation continues to increase in size and cannot be isolated, then the procedure should be aborted and re-attempted in 4 months. Other possible complications associated with maxillary sinus augmentation may include: nerve injury (infraorbital), bruising (ecchymosis), and soft-tissue dehiscence. Careful and meticulous surgical technique is essential to prevent these complications. Infections also may occur (up to 10%) with sinus elevation procedures, and the use of preoperative antibiotics should reduce the risk. Benign paroxysmal positional vertigo has been described as a possible complication after the osteotome internal sinus lift technique. Although the etiology is usually unknown, it is believed that the percussive pressure applied to the maxilla during the osteotome technique could induce the vertigo.33
CONCLUSION
Sinus elevation, with its different modalities for the management of the atrophic posterior maxilla, was described, and the different techniques and materials commonly used were reviewed. It is noteworthy to mention the increased predictability of these procedures as well as the elevated long-term success rate of implants placed in these restored, grafted sites.
REFERENCES
1. McGowan DA, Baxter PW, James J. The Maxillary Sinus and Its Dental Implications.
2. Chanavaz M. Maxillary sinus: anatomy, physiology, surgery, and bone grafting related to implantology—eleven years of surgical experience (1979-1990). J Oral Implantol. 1990;16(3): 199-209.
3.
4. Velásquez-Plata D, Hovey L, Peach C, et al. Maxillary sinus septa: a 3-dimensional computerized tomographic scan analysis. Int J Oral Maxillofac Implants. 2002;17(6):854-860.
5. Wilk RM. Physiology of the maxillary sinus. The physiology of the maxillary sinus as it relates to its functions, mucous membranes, oxygenation, obstruction, and effects of dental procedures is reviewed. Understanding the effects of surgical intervention and disease processes on the physiology of the sinus is essential for managing this area. Oral Maxillofac Surg North Am. 1999;11:(1)15-19.
6. Boyne P, James R. Grafting of the maxillary sinus floor with autogenous marrow and bone. J Oral Surg. 1980;38:(8):613-616.
7. Summers RB. A new concept in maxillary implant surgery: the osteotome technique. Compend Contin Educ Dent. 1994;15(2):152-158.
8. Hirschfeld L, Wasserman B. A long-term survey of tooth loss in 600 treated periodontal patients. J Periodontol. 1978;49(5):225-237.
9. Goldman MJ, Ross IF, Goteiner D. Effect of periodontal therapy on patients maintained for 15 years or longer. A retrospective study. J Periodontol. 1986;57(6):347-353.
10. Laine F. Diagnostic imaging of the maxillary sinus. Oral Maxillofac Surg North Am. 1999;11(1):45-67.
11. Jaffin RA, Berman CL. The excessive loss of Brånemark fixtures in type IV bone: a 5-year analysis. J Periodontol. 1991;62(1):2-4.
12. Chiapasco M, Rosenlicht J, Ruggiero S, et al. The Sinus Bone Graft. 2nd ed.
13. Jensen OT. The Sinus Bone Graft.
14.Fugazzotto P. Augmentation of the posterior maxilla: a proposed hierarchy of treatment selection. J Periodontol. 2003;74(11):1682-1691.
15.Minsk L. Maxillary sinus elevation procedures for endosseous dental implants. Compend Contin Educ Dent. 2004;25(9):672-678.
16.Vercellotti T, De Paoli S, Nevins M. The piezoelectric bony window osteotomy and sinus membrane elevation: introduction of a new technique for simplification of the sinus augmentation procedure. Int J Periodontics Restorative Dent. 2001;21(6):561-567.
17.Wallace SS. Maxillary sinus augmentation: evidence based decision making with biological surgical approach. Compend Contin Educ Dent. 2006;27(12):662-669.
18.Schlee M, Steigmann M, Stom M, et al. Piezosurgery: basics and possibilities. Implant Dent. 2006;15(4):334-340.
19.Zitzmann N, Schärer P. Sinus elevation procedures in the resorbed posterior maxilla. Comparison of the crestal and lateral approaches. Oral Surg Oral Med Oral Pathol Oral Endod. 1998;85(1):8-17.
20.Rosen PS, Summers R, Mellado JR, et al. The bone-added osteotome sinus floor elevation technique: multicenter retrospective report of consecutively treated patients. Int J Oral Maxillofac Implants. 1999;14(6):853-858.
21.Wallace S, Froum S. Effect of maxillary sinus augmentation on the survival of endosseous dental implants. A systematic review. Ann Periodontol. 2003;8(1):328-343.
22.Cammack G, Nevins M, Clem D, et al. Histologic evaluation of mineralized and demineralized freeze-dried bone allograft for ridge and sinus augmentations. Int J Periodontics Restorative Dent. 2005;25(3):231-237.
23.Melcher AH. On the repair potential of periodontal tissues. J Periodontol. 1976;47(5):256-259.
24.Misch CM. The pharmacologic management of maxillary sinus elevation surgery. J Oral Implantol. 1992;18(1):15-23.
25.Misch CE. Contemporary Implant Dentistry. 2nd ed.
26.Laskin D, Dent C, Morris H, et al. The influence of preoperative antibiotics on success of endosseous implants at 36 months. Ann Periodontol. 2000;5(1):166-174.
27.Misch CE, Moore P. Steroids and the reduction of pain, edema and dysfunction in implant dentistry. Int J Oral Implantol. 1989;6(1):27-31.
28.Löe H, Schiott C. The effect of mouthrinses and topical application of chlorhexidine on the development of dental plaque and gingivitis in man. J Periodontol Res. 1970;5(2):79-83.
29.Cohen ES, ed. Atlas of Cosmetic and Reconstructive Periodontal Surgery. 3rd ed.
30.Emmerich D, Att W, Stappert C. Sinus floor elevation using osteotomes: a systematic review and meta-analysis. J Periodontol. 2005;76(8):1237-1251.
31.Cho SC, Wallace SS, Froum SJ, et al. Influence of anatomy on Schneiderian membrane perforations during sinus elevation surgery: three-dimensional analysis. Pract Proced Aesteth Dent. 2001;13(2):160-163.
32.Vlassis JM, Fugazzotto PA. A classification system for sinus membrane perforations during augmentation procedures with options for repair. J Periodontol. 1999;70(6):692-699.
33.Di Girolamo M, Napolitano B,
About the Authors
Fred F. Farhat, DDS, Diplomate of the American Board of Periodontology; Private Practice in Periodontics and Implant Dentistry,
Bassam Kinaia, DDS, MSD, Periodontal Resident,
Howard B. Gross, DDS, MSD, Diplomate of the American Board of Periodontology; Clinical Assistant Professor,
 Figure 1A through Figure 1C Buccal and radiographic views of posterior edentulism with significant sinus pneumatization in the molar region. Figure 1A through Figure 1C Buccal and radiographic views of posterior edentulism with significant sinus pneumatization in the molar region. |  |  |
|
Figure 1D Lateral wall osteotomy. |  Figure 1E The osteotomy was grafted with particulate bone. Figure 1E The osteotomy was grafted with particulate bone. | 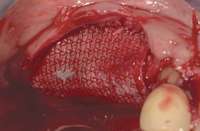 Figure 1F The surgical site was covered with a resorbable barrier. Figure 1F The surgical site was covered with a resorbable barrier. |
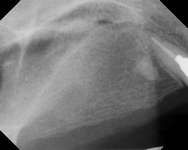 Figure 1G Radiographic confirmation of bone regeneration 8 months after surgery. Figure 1G Radiographic confirmation of bone regeneration 8 months after surgery. |  Figure 1H Radiographic confirmation of implant osteointegration into the new bone 14 months after the initial surgery. Figure 1H Radiographic confirmation of implant osteointegration into the new bone 14 months after the initial surgery. |  Figure 1I. Final implant-supported restoration. Figure 1I. Final implant-supported restoration. |
 Figure 2A Antrostomy performed using piezoelectric surgery, leaving an intact sinus membrane. Figure 2A Antrostomy performed using piezoelectric surgery, leaving an intact sinus membrane. |  Figure 2B Particulate bone graft was placed to lift sinus floor. Figure 2B Particulate bone graft was placed to lift sinus floor. |
|
 Figure 3A Ridge-split osteotomy with lateral wall expansion. Figure 3A Ridge-split osteotomy with lateral wall expansion. |  Figure 3B Particulate bone graft was applied, and simultaneous implant placement was performed. Figure 3B Particulate bone graft was applied, and simultaneous implant placement was performed. |  Figure 3C The site was covered with barrier membrane. Figure 3C The site was covered with barrier membrane. |
 Figure 3D The site 6 months after surgery, confirming integration. Figure 3D The site 6 months after surgery, confirming integration. |  Figure 4A Preoperative radiograph showing ridge resorption. Figure 4A Preoperative radiograph showing ridge resorption. |
|
 Figure 4C Radiographic view of implant placed simultaneously with sinus bone grafting in site No. 3. Figure 4C Radiographic view of implant placed simultaneously with sinus bone grafting in site No. 3. |  Figure 4D Radiographic confirmation of the re-establishment of the sinus floor. Figure 4D Radiographic confirmation of the re-establishment of the sinus floor. |  Figure 4E Final implant-supported restoration. Figure 4E Final implant-supported restoration. |
 Figure 5A Sinus septum evident at site No. 3. Figure 5A Sinus septum evident at site No. 3. |  Figure 5B First, the sinus septum was identified. Figure 5B First, the sinus septum was identified. |  Figure 5C Then, the septum was isolated. Figure 5C Then, the septum was isolated. |
 Figure 5D Lastly, the septum was managed. Figure 5D Lastly, the septum was managed. |
|

 Figure 2C Radiographic confirmation of graft localization to the desired site before membrane application and wound closure.
Figure 2C Radiographic confirmation of graft localization to the desired site before membrane application and wound closure. Figure 4B Radiographic confirmation of graft confinement and incremental addition.
Figure 4B Radiographic confirmation of graft confinement and incremental addition. Figure 5E Bong graft was placed in the mesial and distal compartments.
Figure 5E Bong graft was placed in the mesial and distal compartments.