You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
The stability of the peri-implant bone foundation is fundamental for dental implant success. In many cases, bone volume is insufficient and bone grafting is needed to prepare the implant bed for subsequent implant placement. Guided bone regeneration (GBR) is a highly predictable treatment in dental implantology. The success of the technique is based on several biologically supported principles, summarized with the acronym "PASS": primary wound closure to ensure undisturbed and uninterrupted wound healing, angiogenesisto provide necessary blood supply and undifferentiated mesenchymal cells, space maintenance/creation to facilitate adequate space for bone ingrowth, and stabilityof the wound and implant to induce blood clot formation and uneventful healing events.1
Many successful cases have been described to obtain this goal using various approaches, such as direct implant placement and use of a titanium-reinforced membrane2,3 as well as the use of allograft customized bone blocks.4 Another treatment option to improve bone volume is the use of titanium meshes.5
Facilitating Ridge Augmentation
Titanium is resistant to corrosion, has good mechanical properties, is very strong, and is stiff enough to enable support for a bone graft to maintain its volume during healing.6 The use of titanium mesh facilitates ridge augmentation in vertical and buccal directions before or simultaneous with implant placement. The integration of the graft typically is excellent with only minimal bone resorption because the titanium mesh protects the graft from exterior trauma and nonfunctional forces.7
Since von Arx introduced the TIME technique (autogenous bone grafting combined with stabilization using a titanium mesh) and conducted his research on titanium mesh in 1996, the use of this device has undergone different stages, with clinical procedures continuously evolving to shorten surgery time, reduce patient trauma, and increase the success rate of bone augmentation.8 A recent study showed good results with vertical ridge augmentation with titanium-reinforced polytetrafluoroethy- lene (PTFE) mesh using a mixture of auto-logous bone and xenograft. In these patients, the area to be covered by mesh was estimated, and an appropriately sized titanium-reinforced PTFE mesh was selected, trimmed, and placed to completely cover the graft and at least 2 mm of adjacent native bone.9
The main disadvantage of such prefabricated titanium meshes is the intraoperative and time-consuming manual shaping, which is based on the individual defect size of the patient. With modern computer-aided design/computer-aided manufacturing (CAD/CAM) technology, however, the clinician can now design patient- customized meshes and calculate how much bone is needed to rebuild lost hard tissue based on a cone-beam computed tomography (CBCT) or CT scan. Virtual planning of the mesh requires advanced knowledge of anatomical as well as implant considerations. The use of this CAD/CAM-based approach can eliminate the need for intraoperative trimming of the prefabricated titanium scaffolds, reducing morbidity, costs, and surgery time.10,11
In the following two cases, the patients presented with severe ridge atrophy and a need for bone augmentation. Using CBCT and CAD/CAM, titanium meshes were designed for vertical and horizontal ridge augmentations. (Both patients signed informed consent statements.)
Case 1
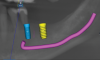
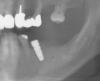
Patient 1 was a 69-year-old man who was a former professional athlete. He developed heart issues, which led to the use of various medications, such as metoprolol, Ventolin, Seretide, pantoprazole, Rhinocort, and Eliquis. Based on a CBCT scan (Figure 1), the patient needed augmentation in the mandibular left jaw (Siebert class I). Radiographic examination revealed a periapical lesion present at site No. 20 as well as a very thin ridge width of only 3.7 mm in the posterior mandible. Implant planning was performed using planning software, and a custom-made titanium mesh was designed (Figure 2).12
The patient received amoxicillin 500 mg 3 times a day for 10 days, starting the day before surgery.13,14 A full-thickness flap was elevated, extending from tooth No. 22 to at least one tooth mesial and distal to the mesh placement area (Figure 3). Although a vertical releasing incision was not necessary mesially, one can be made to allow sufficient tissue and ensure tension-free closure. It is important that the vertical incision does not end at the joint between the host bone and mesh. The periosteum in this case was left intact and no superficial release of the mylohyoid lingual was necessary.3,15,16
Implant and Mesh Placement
Tooth No. 20 was extracted atraumatically and the extraction site was thoroughly degranulated. An implant with platform-switching (10 mm length) was placed directly in the extraction socket. The socket was filled with particulate allograft, which was also used to fill the mesh. The receptor site was perforated with a 1.1-mm diameter round bur, but not at the places where the fixation screws would need to be placed.
After implant placement, the mesh was secured in place. Special care was taken to ensure that pre-designed fixation holes did not align with anatomical sensitive areas. The mesh was loaded with the grafting material and placed over the implant. It was fixated with two screws (1.2 mm x 6 mm) designed within the mesh, as planned (Figure 4).
A pericardium membrane was placed. It covered the entire site and extended 2 mm to 3 mm from the mesh margins so it could be secured with tacks and sutures at both the oral and labial surfaces. The membrane was placed under tension to completely cover the grafted site. The flap was advanced and sutured without tension using simple interrupted sutures (Figure 5). At least 6 to 8 months would be allowed for healing to occur.17 A premature loading was avoided; therefore, no interim prosthesis over the grafted site was used.
Clinical follow-ups at 2 and 7 days post- surgery were performed and did not show any complications. Sutures were removed after 14 days. During the healing period, the mesh became slightly exposed (Figure 6), and the patient was instructed to clean the exposed area with chlorhexidine on a cotton tip (twice a day) to keep the area clean.
Re-entry and Mesh Removal
After 5.5 months, a new CBCT was made, which showed good-quality bone around the implant. Before mesh removal, a 500 mg 3 times a day 7-day amoxicillin regimen was given, starting 1 hour before surgery. After flap release (Figure 7), the mesh was removed and the implant was found to be covered crestally by solid bone, which was removed in order to place the healing abutment (Figure 8).
To improve the soft-tissue phenotype, a soft-tissue graft was placed over the implant.18 The flap was closed with conventional interrupted sutures and a healing abutment was placed (Figure 9 and Figure 10).
Case 2
Patient 2, a 50-year-old woman with minor osteoporosis, needed grafting because of severe atrophy in the right mandible (Siebert class II) (Figure 11 and Figure 12). The titanium mesh mesh was designed using CAD/CAM tech- nology in the same manner as in Case I. In this case, a mix of autologous and xeno- graft was used. Re-entry time was 8 months. The same protocol was followed as in Case 1 (Figure 13 through Figure 17).
A CBCT was made before re-entry, revealing good-quality bone underneath the titanium mesh (Figure 18). The mesh was removed, two implants (4.1 mm and 4.7 mm diameter) were placed (Figure 19), and the flap was closed with conventional interrupted sutures (Figure 20 and Figure 21).
Results
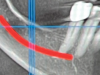
In each case, a CBCT was taken prior to mesh removal. Through the use of the measurement tool of the planning software, a calculation of the amount of bone gained was done. Patient 1 showed 4.1 mm vertical gain and a width of 8.7 mm (Figure 22). Patient 2 presented 6.7 mm vertical gain and a 10.8 mm width (Figure 23).
Discussion
The TIME technique has been a successful procedure for localized alveolar ridge augmentation.7 The use of a strong titanium mesh facilitates bone formation for ridge augmentation in horizontal and vertical ridge deficiencies. The integration of the graft is well condensed with only minimal bone resorption because the mesh protects the grafting material particles from exterior trauma and nonfunctional forces. Titanium has excellent tissue compatibility and provides long-term bone graft stabilization.7New digital protocols, including the production of patient-specific titanium meshes, resorbable membranes, and bone grafting materials, have proven to be promising techniques for the private practice.19
The use of a titanium mesh scaffold in combination with autologous and/or heterologous particulate grafts represents a safe and predictable treatment to increase vertical and/or horizontal bone volume in cases with ridge deficiencies in partially edentulous patients, the treatment of small- and medium-sized defects around dental implants, and alveolar ridge preservation after tooth extraction. However, usage of the mesh presents drawbacks related to the need for a second-stage surgical procedure, thereby increasing patient morbidity and rehabilitation time. Furthermore, a high risk of soft-tissue dehiscence and membrane exposure exists.20 Lack of exposure is undoubtedly an essential factor for graft vitality and alveolar ridge reconstruction, as exposure may make the membrane vulnerable to oral flora, increasing the risk of infections and, consequently, lack of revascularization. Also, exposure can lead to the invasion of epithelial cells into the graft through the pores of the mesh.20-22
Exposure of titanium mesh is well-researched; in a review of 677 surgical sites, 225 cases of mesh exposure were identified, for an exposure rate of 33.3%.23 Eleven treatments have been described for dealing with mesh exposure. Chlorhexidine was the first approach, used in 46% of cases. Oral hygiene instructions and follow-up was second, with 22.5% of occurrences. In 21% of clinical situations, removal of the titanium mesh was the treatment of choice, associated with other measures (namely, administration of antibiotics). There seems to be a consensus in cases of infection in that, when exposure happens and there is tissue dehiscence, the primary treatment is mesh removal. The same does not occur when the site needs to be cleaned for long-term periods. No changes in treatment have occurred over the past 20 years.23,24
When a dehiscence occurs, it typically appears around the sutures. Therefore, positioning the margin of the wound in the vestibulum and in a distance from the mesh seems to reduce the risk for an exposure of the mesh, as the margin of a wound represents the most important nutritional structure for survival and the basis for reliable wound healing.25 In the present cases, the mesh was subsequently covered with a collagen membrane. Recent research by Cucchi et al showed that customized meshes alone do not appear to be inferior to customized meshes covered by cross-linked collagen membranes in terms of healing complication rate and regeneration rate; however, a trend of more favorable clinical results was observed when a membrane was used.24Another study, though, suggested improved soft-tissue healing with the use of resorbable membranes and advanced-platelet rich fibrin (A-PRF) clot.19Mesh exposure was also recently researched by Gu et al, who found a 21.7% exposure rate; they also concluded that it did not seem statistically significant as to the type of resorbable membrane or graft material used.26
An interesting issue also observed in the present cases was the difficulty in removing the mesh due to the peripheral margins of the mesh being embedded in newly formed bone and fibrous adherences. Removal of meshes placed in the posterior mandible is especially challenging on the lingual side because of the attachment of the mylohyoid muscle and fibrous adherences to the mesh.24Consideration, therefore, should be given to the use of a previously or simultaneously placed keratinized tissue graft or Kazanjian vestibuloplasty technique to eliminate the muscular insertion and movements of soft tissue for the long-term success of the graft and implant.27
Guided implant surgery using computer- designed stereolithographic guides is a reliable technique when taking into account the mean accuracy, but if the maximum deviation is considered, the same technique appears far from accurate. Clinicians should be alert near vital structures, and a minimum of at least 2 mm distance from these anatomical structures should be respected.28
These novel techniques are often described as "risk-free" and easy to use. Computer-guided implantology, however, does not overcome all limitations and should only be used by experts to achieve improved results. A typical learning curve effect was not identified for static computer-assisted implant surgery.29
In the first patient, an implant was placed simultaneously with GBR, saving time with regard to placement of allograft customized bone blocks, which also can be used to gain vertical bone height.4 Implant survival and success rates are similar for implants placed in native bone and when performing other GBR techniques. Also, there is no difference in implant survival and success when comparing simultaneous and delayed implant placement.20
Conclusion
Within the limitations of this two-case report, the results show that procedures utilizing customized CAD/CAM-designed titanium meshes are safe and predictable for large vertical and horizontal ridge augmentations, which can be combined with direct implant placement. With the combination of both allograft and xenograft materials there were predictable results. Soft-tissue coverage remains one of the most critical steps when using this technique. Additionally, exposure of the mesh does not appear to affect the clinical outcome of this technique.
Acknowledgment
The CBCT analysis and mesh design were performed by Stefan Berger, PhD.
Disclosure
The authors declare no conflicts of interest.
About the Authors
Maarten J. Boogaard, DMD
Private Practice, Amsterdam, The Netherlands
Fausto Santoro, DDS
Private Practice, Milan, Italy
Georgios E. Romanos, DDS, PhD, Prof Dr med dent
Professor, Department of Periodontology, School of Dental Medicine, Stony Brook University, Stony Brook, New York; Professor, Department of Oral Surgery and Implant Dentistry, Johann Wolfgang Goethe University, Frankfurt, Germany
Queries to the author regarding this course may be submitted to authorqueries@broadcastmed.com.
References
1. Wang HL, Boyapati L. "PASS" principles for predictable bone regeneration. Implant Dent. 2006;15(1):8-17.
2. Ronda M, Rebaudi A, Torelli L, Stacchi C. Expanded vs. dense polytetrafluoroethylene membranes in vertical ridge augmentation around dental implants: a prospective randomized controlled clinical trial. Clin Oral Implants Res. 2014;25(7):859-866.
3. Ronda M, Stacchi C. A novel approach for the coronal advancement of the buccal flap. Int J Perio- dontics Restorative Dent. 2015;35(6):795-801.
4. Boogaard MJ, Romanos GE. Allograft custom- ized bone blocks for ridge reconstruction: a case report and radiological analysis. Appl Sci. 2021;11:10413. https://doi.org/10.3390/app112110413.
5. von Arx T, Kurt B. Implant placement and simultaneous ridge augmentation using autogenous bone and a micro titanium mesh: a prospective clinical study with 20 implants. Clin Oral Implants Res. 1999;10(1):24-33.
6. Jung GU, Jeon JY, Hwang KG, Park CJ. Preliminary evaluation of a three-dimensional, customized, and preformed titanium mesh in peri-implant alveolar bone regeneration. J Korean Assoc Oral Maxillofac Surg. 2014;40(4):181-187.
7. von Arx T, Hardt N, Wallkamm B. The TIME technique: a new method for localized alveolar ridge augmentation prior to placement of dental implants. Int J Oral Maxillofac Implants. 1996;11(3):387-394.
8. Xie Y, Li S, Zhang T, et al. Titanium mesh for bone augmentation in oral implantology: current application and progress. Int J Oral Sci. 2020;12(1):37.
9. Urban IA, Saleh MH, Ravida A, et al. Vertical bone augmentation utilizing a titanium-reinforced PTFE mesh: a multi-variate analysis of influencing factors. Clin Oral Implants Res. 2021;32(7): 828-839.
10. Sumida T, Otawa N, Kamata YU, et al. Custom- made titanium devices as membranes for bone augmentation in implant treatment: clinical application and the comparison with conventional titanium mesh. J Craniomaxillofac Surg. 2015;43(10):2183-2188.
11. Ciocca L, Ragazzini S, Fantini M, et al. Work flow for the prosthetic rehabilitation of atrophic patients with a minimal-intervention CAD/CAM approach. J Prosthet Dent. 2015;114(1):22-26.
12. Cruz N, Martins MI, Santos JD, et al. Surface comparison of three different commercial custom-made titanium meshes produced by SLM for dental applications. Materials (Basel). 2020;13(9):2177.
13. Esposito M, Grusovin MG, Worthington HV. Interventions for replacing missing teeth: antibiotics at dental implant placement to prevent complications. Cochrane Database Syst Rev. 2013;2013(7):CD004152.
14. Canullo L, Troiano G, Sbricoli L, et al. The use of antibiotics in implant therapy: a systematic review and meta-analysis with trial sequential analysis on early implant failure. Int J Oral Maxillo- fac Implants. 2020;35(3):485-494.
15. Romanos GE. Periosteal releasing incision for successful coverage of augmented sites. A technical note. J Oral Implantol. 2010;36(1):25-30.
16. Abed PF, El Chaar E, Boltchi F, Bassir SH. The novel periosteal flap stretch technique: a predictable method to achieve and maintain primary closure in augmentative procedures. J Int Acad Periodontol. 2020;22(1):11-20.
17. El Chaar E, Urtula AB, Georgantza A, et al. Treatment of atrophic ridges with titanium mesh: a retrospective study using 100% mineralized allograft and comparing dental stone versus 3D-printed models. Int J Periodontics Restorative Dent. 2019;39(4):491-500.
18. Farina V, Zaffe D. Changes in thickness of mucosa adjacent to implants using tissue matrix allograft: a clinical and histologic evaluation. Int J Oral Maxillofac Implants. 2015;30(4):909-917.
19. Hartmann A, Seiler M. Minimizing risk of customized titanium mesh exposures - a retrospective analysis. BMC Oral Health. 2020;20(1):36.
20. Aceves-Argemí R, Roca-Millan E, González-Navarro B, et al. Titanium meshes in guided bone regeneration: a systematic review. Coatings. 2021;11(3):316. https://doi.org/10.3390/coatings11030316.
21. Lizio G, Corinaldesi G, Marchetti C. Alveolar ridge reconstruction with titanium mesh: a three-dimensional evaluation of factors affecting bone augmentation. Int J Oral Maxillofac Implants. 2014;29(6):1354-1363.
22. Her S, Kang T, Fien MJ. Titanium mesh as an alternative to a membrane for ridge augmentation. J Oral Maxillofac Surg. 2012;70(4):803-810.
23. Cunha G, de Azambuja Carvalho PH, Cabrini Gabrielli MA, et al. Titanium mesh exposure after bone grafting: treatment approaches-a systematic review. Craniomaxillofacial Trauma & Reconstruction. 2022;15(4):397-405.
24. Cucchi A, Vignudelli E, Franceschi D, et al. Vertical and horizontal ridge augmentation using customized CAD/CAM titanium mesh with versus without resorbable membranes. A randomized clinical trial. Clin Oral Implants Res. 2021;32(12): 1411-1424.
25. Kleinheinz J, Büchter A, Kruse-Lösler B, et al. Incision design in implant dentistry based on vascularization of the mucosa. Clin Oral Implants Res. 2005;16(5):518-523.
26. Gu C, Xu L, Shi A, et al. Titanium mesh exposure in guided bone regeneration procedures: a systematic review and meta-analysis. Int J Oral Maxillofac Implants. 2022;37(1):e29-e40.
27. Khoury F, Antoun H, Missika P. Bone Augmentation in Oral Implantology. Berlin: Quintessence Publishing; 2007:XV,520 S.
28. Cassetta M, Stefanelli LV, Giansanti M, et al. Accuracy of a computer-aided implant surgical technique. Int J Periodontics Restorative Dent. 2013;33(3):317-325.
29. Cassetta M, Giansanti M, Altieri F, et al. Is there a learning curve in static computer-assisted implant surgery? A prospective clinical study. Int J Oral Maxillofac Surg. 2020;49(10):1335-1342.