You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
Historically in case planning for and performance of restorations, practitioners used analog techniques, including impressions, caps, loose alginate models, duplicate clear dentures with cutouts, and observations in the operatory to create restorations using traditional approaches. These methods did not allow advance visualization of the end result-with the practitioner essentially guessing by figuring out steps along the way. Surgical approaches ranged from freehand to printed remote guides and guided surgery to navigational surgery.1
Different sizes and the challenges of complex cases required differing levels of foresight, treatment planning, and build-out before surgery. Cases requiring restorations over large "territory" could become confusing because visual references often were sacrificed or eliminated when progressing through a full-mouth extraction and implant case. With only a limited treatment plan and surgical guidance protocol achievaable through older technology, providers sometimes provided treatment based on limited knowledge, with many adjustments required on the spot.1
Because restorations often involve irreversible surgical procedures, planning must be performed as conscientiously and successfully as possible. Robotic technology brings new advantages to assure that practitioner promises to patients are fulfilled and allow practitioners to leverage technology to its fullest.2-4
Guide Usage: Previous "Gold Standard" Not So Golden
Guides are printed or milled plastic surgical templates that fit into the mouth; they can be simple, single-piece guides or stackable systems that reference existing teeth and build a platform crucial to implant and bone reduction procedures, and they can even reference the position of the temporaries for pickup and direct immediate loading (Figure 1). However, although guides were previously considered the technological "gold standard" for dental implant surgery, they actually constitute a complex and cumbersome means to an end, requiring a large amount of preparation, parts, effort, and cost before surgery occurs.5-7 Multiple layers of potential error and inaccuracies that can occur with a guide include how well the data files are aligned, how well the design file is produced by the 3D printer, how well it is post-processed and cured, and how accurate it is in reality versus planning. Another problem is the potential difference between dental anatomy at the time of procedure versus when it was captured with the scan. Teeth often cannot be trusted as solid points of anchorage and indexing, particularly when compromised.8
Another potential problem is how well the guide has been constructed, including how well drill guide sleeves have been inserted and bonded or glued into place. Guides may become distorted and break as pieces are fitted onto other pieces. Each element of a guide system has necessary "wiggle room" built into it to allow for stacking, but stacking the elements together compounds the wiggle room, such as when there is a tooth-borne vestibular pin guide and an implant guide on top of it is indicated. Guides may not fit together well out of the printer, or they may be too thin. Sometimes elements must be inserted at an awkward angle; a pin guide may break or pop out in the middle of surgery. Parts that are not supposed to move may do so anyway. Modality for error amplifies exponentially with level of complexity.7
Robotic technology, however, minimizes and even eliminates modality for errors associated with the standard of care by eliminating steps and allowing the practitioner to implement the coordinate data directly referenced to the patient anatomy, saving not only time and money but the risk of inaccurate surgery.2-4
Even in a generally straightforward dental implant scenario, such as a posterior dental implant or premolar with adequate bone, there can be challenges with static guides, such as unrecognizable anatomy on a 3D x-ray and questions about reliable surface data to overlay an intraoral or model scanner (Figure 2). The practitioner still must proceed with treatment planning and pick out guide sleeves; the guide sleeve position, and therefore the implant position, is only as accurate as the file merger from the beginning of the treatment plan. Often it is not accurate; there is a lot of "slop" built into the gateways to getting a guide manufactured. Practitioners still must visually verify how well files are aligned.9
Practitioners must decide what kind of guide sleeve to use, and new ones must be purchased for every new guide, with no guarantee that the sleeves will even fit in the particular patient's anatomy. Sometimes there are space constraints that limit what the practitioner can actually accomplish through guided surgery protocols. The practitioner may downsize the guide sleeve and then use an osteotomy drill in an unguided manner to enlarge the osteotomy so that an implant can be placed in the site. He or she may do also a pilot hole and finish the surgery by hand-eye coordination alone.9
Even if a guide is perfectly oriented, conceived, and produced, it is only as accurate as the initial file superimposition and may not account for all the compromises the practitioner will require, such as accomplishing procedures in human anatomy with enough room for an added 10 mm of drill shank length typical for a guided surgery drill kit. A robotic system mitigates the need for an extra link to the drills and limited access to accomplish posterior implant placement because it allows the practitioner to use a straight short shank surgical drill kit without a static guide.2-4
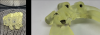
In the case of a two mandibular overdenture surgical plan, a bone fixation pin would be the means of stabilizing the guide throughout the procedure. Much data are required to make sure that every bit of the physical object can be made from the digital file, with many printer supports so the guide can be produced layer by layer through the stereolithographic (STL) process. It comes out of the printer covered in excess resin that must be removed (Figure 3). The resin must be post-cured to achieve final rigidity. After post-curing, print supports must be clipped away, sometimes taking pieces of the guide away with them. Only then are the metal sleeves inserted and bonded into place (Figure 4); sometimes the sleeves protrude through the tissue-contacting surface guides, requiring grinding after the fact to assure a fit into the patient's mouth.10
A variety of supplies and tools are required to deal with the potential and actual errors, and much time and cost is required to manage the 3D printing and post-processing. Robotic technology eliminates these as well.2-4
Navigational Dental Implant Surgery
Another technology is navigational dental implant surgery. It offers drilling precision and visual orientation that is better than standard freehand procedures.5,6 However, it requires not only hand-eye coordination for procedures in the mouth, but also coordination with the computer screen. Practitioners are required to look directly at the computer screen more than at the surgical field. The practitioner is forced to try to "target the bullseye," with nothing physically guiding the hand other than his or her own dexterity.7
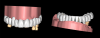
Practitioners need precision and accuracy, require procedures to be repeatable, and must know whether there will be similar errors in a similar direction for a full-arch dental implant (Figure 5). Tying implants together as a system, as an arch form foundation or arch form of teeth, and then coming close to the bullseye is not good enough in connecting a whole arch form to the foundation. It is necessary to spend time doing a workup ahead of surgery in order to spend less time during surgery and to be systematically in control of any margin of error. Navigational dental implant surgery leaves too much to the eye and hand, disrupting the overall accuracy of the system.7
Robotic Technology Workflow
Robotic technology provides a confluence of concepts and attributes that may be somewhat lacking when using static guides and navigational implant surgery; robotics offer complete visual and surgical access to a site and physical, haptic guidance in the practitioner's hands, allowing him or her to stay on plan.2-4 There is currently one FDA cleared robotic-assisted dental surgery system in the United States.11
Robotic technology may be used for simple and complex cases, including full-arch treatment. It allows a workflow similar to that of virtual surgical planning or planning for clear aligners; all the records are taken digitally, and the practitioner can create a digital design or outsource the planning to a digital design center. In either case, a digital review is indicated. The review will determine which items must be digitally fabricated, such as a provisional crown for an implant, a denture, a fixed prosthesis, or other applications, and will show where implants or restorations will be placed.2-4
The robust capabilities of robotic technology include versatile treatment planning software. Procedure planning can be done in advance on any PC available to the practitioner and the plan can be altered at any time, even during surgery if needed. The practitioner can build virtual versions of patients as they are in the present and then build virtual and multiple versions of them as they may be in the future; then these versions can easily be shown to patients through images on a screen. The technology can help patients understand the procedures and how they can be achieved; meanwhile, the practitioner is obtaining patients' acceptance and trust.2-4
After the practitioner adjusts or approves the design, the information is uploaded into the robot so it is fully ready for surgery, at which point it is registered to the patient anatomy through a splint and tracking arm. Robotic technology bridges the gap between just creating and inspecting a plan or creating a static guide and actually physically guiding the delivery of the care digitally.2-4
Robotic-assisted dental surgery combines the advantages of both the physical constraints of static guides and the flexibility of image-based dynamic navigation. Haptic technology allows the practitioner to move the robotic handpiece just as he or she would move a traditional handpiece, with the added benefit of physical feedback that provides extra guidance. Robotic assistance provides 3D physical guidance of the dental surgical instruments during execution of the digital plan in terms of the desired location, angulation, and depth of the osteotomy. Surgery is performed through the robot, precisely as it was designed in the virtual world without static guides. The practitioner gets a visual readout, with coordinate data input to the robot, without having to lift his or her eyes from the surgical field. Predicted results seen on-screen become reality. The use of robotics minimizes stack-up errors commonly found with static guides and while utilizing the practitioner's familiarity with digital planning and surgical and restorative processes. Practitioners build rapport with patients through delivering on promises made, increasing patient confidence, and providing esthetically satisfying and functional restorations.2-4
Because of the precision and accuracy that robotics offers, it is growing in dentistry and is expected to expand to other areas, such as orthognathic and temporomandibular joint surgery, restorative dentistry functions such as crown preparations, and endodontics. Robotics may make practitioners technically better treatment planners, dentists, and surgeons, perhaps someday becoming the standard of care.2-4
Case Examples
In the case of an edentulous patient, in the virtual surgical planning realm practitioners typically overlay computed tomography (CT) scans for treatment planning purposes and can do so in multiple software platforms (Figure 6). Robotic technology has the same capability to track radiopaque markers, such as gutta percha or global composite.12
The dots between the arches on a CT scan are reference points that are valuable in treatment planning to coordinate data and visualize results to form a blueprint to use in laying the foundation and finding an anatomically correct location for implants (Figure 7). The result is a concerted plan that ends with good results in a predictable manner because the technology allows the practitioner to see everything during planning and surgery. It is not complicated, can happen in the same day, does not involve a protracted treatment planning process, and affords the flexibility to make changes intraoperatively, allowing the practitioner to see where changes would impact not just the patient anatomy, but the prosthetic anatomy.3,4
In a more complicated case, often there are more complicated starting points. The patient shown in Figure 8 had bite posture problems, caries, periodontal disease, failing restorations and implants, and a history of head-and-neck cancer. Such a patient may logically fear the unknowns of treatment, but with the treatment planning and rendering capabilities robotics provide, the practitioner could determine exactly what the patient needed, convey the information to the patient, and deliver promised results.
In such a patient, there may be little or no dental topography or teeth with which to work. The CT scan shows only the bony structure, which is what the practitioner is concerned with regarding dental implants, but from a treatment plan standpoint, the practitioner needs to visualize the way through and unwind the complex layers of such a puzzle. Robotics allow the practitioner to employ software on the front end and optimized for the robotic surgical approach in the middle, making the back-end treatment much easier. Scanning templates allow alignment of intraoral scans; the practitioner can add that result with high fidelity back to a CT scan that may otherwise have been unusable (Figure 9). The practitioner also can add other layers, including facial images to start building an improved version of the patient smile. With the data put into the robotic system, the plan is validated with easier to use digital versions that replace older analog treatment planning procedures involving alginate, stone models, articulators, and wax-ups.1-4
With robotics, whether for a simple one-implant procedure or a complicated overdenture or fixed attachable restoration procedure, the steps are the same, starting with aligning data in the robotic software from a treatment plan standpoint. In a case lacking trustworthy teeth, for example, the practitioner can align separate STL files relative to a patient x-ray (Figure 10) and have a blueprint on the screen so that, when designing the implants foundation for yet-to-be-achieved teeth, he or she knows that they will line up.3,4
The practitioner can export virtually a line scan and overlay it with a digital surgical model of teeth relative to ideal teeth verified virtually in the patient's face (Figure 11). The practitioner can essentially have the "master cast" on the front end versus the back end, not needing to wait until he or she has inserted the implants and then be forced to make a bloody impression the day of surgery or have to bring the patient back a different day. The practitioner has the information in advance of surgery.3,4
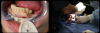
A patient tracker arm attaches directly to the patient's bony structure via surgical splint fitting deep down into the vestibular area. With threaded screws, it fixates more solidly than a surgical guide and is rigidly secured to the patient (Figure 12). This allows registration of the robot and the plan to the patient's anatomy and enables the handpiece of the robotic system to help the practitioner deliver the osteotomy and eventually the implant, unobstructed by multiple layers of printed plastic and unimpeded for irrigation, visual access, and bone reduction.2-4
Considering that the phases of treatment are diagnostics, surgery, restoration, and maintenance: the robotic system's diagnostics are superb, surgical standards are elevated, the restoration phase gets easier, and the maintenance phase is less complex and problem prone. With digital technology, all aspects are represented 3-dimensionally on the computer; therefore, practitioners can proceed far down the diagnostic treatment planning track before physically committing themselves or their patients to any part of the process, allowing more informed treatment and financial decisions.2-4
Case Planning
In the preoperative phase, when the patient comes in for an appointment, removable teeth are cleared away, the oral cavity is scanned, and the face is databased through a high-resolution diagnostic video. Within 60 seconds, the practice can harvest out any still image needed to begin treatment planning, allowing the practitioner to perform pre-design work based on the data compiled in advance. When trying in what he or she has pre-designed, the practitioner can verify within seconds whether that design work is accurate. If it is not, he or she can make real-time changes. The practitioner can immediately remove bad teeth and replace them with good temporary teeth (Figure 13), getting both practitioner and patient fast-tracked to discussing implants and planning surgery.
Going from virtual to reality, topographical landmarks on the bony surfaces are used as 3D blueprints for implant planning. Every bit of information needed is on the screen (Figure 14) and is verified, allowing rendering of a surgical result with a degree of precision not possible with computer-based planning. Regardless of how complicated the implant planning, the practitioner can concentrate on the oral cavity with the computer screen providing the reference points.2-4
Robotic technology increasingly consolidates patient flow. With dental diagnostics becoming increasingly nonlocalized to dentistry through mobile CT scanning units and teledentistry, robotic technology enables a practice to handle data easily, regardless of where they originate. In addition, with patients becoming savvier about robotic surgery through the media, they are predisposed to favor the practitioner who uses the latest technology.13
The technology in robotics does not take over the treatment of patients. Instead, it allows the practitioner to concentrate more on diagnosis and treatment planning and to be precise and accurate with delivery of care.
Conclusion
Robotic technology in implant surgery offers enhanced digital diagnostics, treatment planning, surgery, restoration, and maintenance, with potential gains in speed and accuracy without adding any complexity or extra steps compared with older analog technologies. It helps to provide patient confidence in the practitioner and reduces patient time spent in the office. It also "future-proofs" the practice by providing the technology to handle data from a wide variety of sources and with which patients are increasingly familiar.
About the Author
Scotty Bolding, DDS, MS
Private Practice, Fayetteville, Arkansas; Director of Oral and Maxillofacial Surgery, PreciDent Center for Dental Medicine, Rogers, Arkansas
Andrew Johnson, DDS, MDS, CDT
Director of Prosthetic Dentistry, PreciDent Center for Dental Medicine, Rogers, Arkansas
References
1. Block M. Dental implants: the last 100 years. J Oral Maxillofac Surg.2018:76(1):11-26.
2. Rawal S, Tillery DE Jr, Brewer P. Robotic-assisted prosthetically driven planning and immediate placement of a dental implant. Compend Contin Educ Dent. 2020;41(1):26-30.
3. Ansari R. Robotically-guided dental implant placement: extending surgical expertise. Oral Health. https://www.oralhealthgroup.com/features/robotically-guided-dental-implant-placement-extending-surgical-expertise/. Published July 24, 2020. Accessed August 18, 2020.
4. Wu Y, Wang F, Fan S, Chow JK. Robotics in dental implantology. Oral Maxillofac Surg Clin North Am. 2019;31(3):513-518.
5. Jung RE, Schneider D, Ganeles J, et al. Computer technology applications in surgical implant dentistry: a systematic review. Int J Oral Maxillofac Implants. 2009;24(suppl):92-109.
6. Vercruyssen M, Fortin T, Widmann G, et al. Different techniques of static/dynamic guided implant surgery: modalities and indications. Periodontol 2000. 2014;66(1):214-227.
7. Block MS, Emery RW. Static or dynamic navigation for implant placement-choosing the method of guidance. J Oral Maxillofac Surg.2016;74(2):269-277.
8. Tolstunov L. Dental implant success-failure analysis: a concept of implant vulnerability. Implant Dent. 2006;15(4):341-346.
9. DeSantis D, Malchiodi L, Cucchi A, et al. The accuracy of computer-assisted implant surgery performed using fully guided templates versus pilot-drill guided templates. BioMed Res Int. 2019;9023548:1-10.
10. Lin CC, Ishikawa M, Maida T, et al. Stereolithographic surgical guide with a combination of tooth and bone support: accuracy of guided implant surgery in distal extension situation. J Clin Med. 2020;9(3):709.
11. Neocis announces new FDA 510(k) clearance enabling the Yomi® dental robotic system to assist with full arch implant treatment [press release].https://www.neocis.com/news/neocis-announces-new-fda-510k-clearance-enabling-the-yomi-dental-robotic-system-to-assist-with-full-arch-implant-treatment/. Published July 28, 2020. Accessed August 18, 2020.
12. Abboud M, Orentlicher G. An open system approach for surgical guide production. J Oral Maxillofac Surg. 2011;69(12):519-524.
13. Shrirao N, Deshmukh SP, Pande NA, Radke UM. An evaluation of patient's decisions regarding dental prosthetic treatment. J Indian Prosth-
odont Soc. 2016;16(4):366-371.