You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
A questionnaire survey of the anesthesia care and prescribing practices of oral and maxillofacial surgeons in the United States in 2006 indicated that opioid-containing analgesics were commonly prescribed following third-molar extraction surgery.1,2 The two formulations most often recommended were hydrocodone with acetaminophen and oxycodone with acetaminophen.2 It was noted that most of the prescriptions for opioid pain relievers (OPRs) included instructions to take the medication “as needed for pain relief.” Although the practitioners prescribed a median dose of 20 tablets (range 8 to 40), the actual number of analgesic tablets that were consumed was not determined.2
As a follow-up to this survey, the authors undertook a structured telephone interview of patient experiences following third-molar extractions. The goal of this patient survey of surgical experiences was to identify and quantify pain severity, analgesic prescribing practices, patient postoperative utilization of OPRs, and complications following intravenous sedation for third-molar extraction surgery. The authors were also interested in determining the patterns of prescribing opioid-containing formulations in light of increasing concerns about abuse of these drugs.3 This assessment was undertaken between July 2012 and August 2013 among patients treated at the University of Pittsburgh School of Dental Medicine’s Departments of Dental Anesthesiology and Oral and Maxillofacial Surgery.
Methods
This prospective survey was completed using a structured postoperative telephone interview. On days 1 and 7 following anesthesia/surgery, patients were called by a dental anesthesiology resident and queried regarding the perceived severity of their postoperative pain, use of prescription OPRs, and complications. The project was reviewed by the University of Pittsburgh’s Institutional Review Board (IRB) and, because it involved no intervention and maintained confidentiality, was approved with exempt status.
For data collection, patients were identified only by their first name and a telephone number where they could be contacted after surgery. Demographic variables (age, weight, gender) and procedural variables (surgical procedure, number of teeth extracted, duration of surgery, anesthetic agents employed, analgesic prescription provided) were collected from anesthesia charts and patient records to supplement the patient telephone responses. The degree of surgical difficulty (DSD) was rated by summing the total number of teeth that were: erupted = 1; partially impacted = 2; or fully impacted = 3. The range of DSD values for four teeth would be calculated as 4 (all teeth erupted) to 12 (all teeth fully impacted).
Patients were called 24 hours and 7 days following surgery. Questions related to “worst level of pain experienced” during each period were categorized as none, mild, moderate, and severe. Use of peripherally acting analgesics was grouped into categories of ibuprofen products, acetaminophen products, and other. Specific questions regarding the patient’s consumption of OPRs and the number of tablets remaining were asked. A global question regarding problems with treatment and recovery included specific inquiries concerning nausea or vomiting, bleeding or oozing, and soreness at the venipuncture site.
Data were coded and entered into a spreadsheet, and descriptive analyses were performed using JMP® Pro 10.0.0 software. Data entry was repeated with 20% of the records to assure accuracy of entry. Factors potentially associated with postoperative pain and analgesic consumption (age, weight, gender, DSD, number of teeth, duration of surgery, specific anesthetic, and adjunctive agents) were explored using pairwise statistics and multiple linear regression analyses.
Results
The final analysis describes the responses provided by 48 patients who participated in this telephone assessment of their postoperative experiences. In the waiting area on the day of surgery, staff of the Department of Dental Anesthesiology contacted 57 patients who were scheduled for third-molar extraction surgery and intravenous sedation. The goal and description of this telephone survey was explained in detail. Three patients declined to participate. Telephone follow-up could not be established for four patients because of staff scheduling difficulties, and telephone contact for two patients was attempted but was unsuccessful at both the 1-day and 7-day follow-up calls.
The remaining 48 participants were included in the final analysis; all 48 were contacted at day 1, and 41 were successfully contacted at 1 week. Of the 48 patients who were included, 32 were female, and 16 were male. Mean age was 19.6 (+/- 0.6 s.e.) years (range 15 to 30 years). Mean weight was 143.0 (+/- 4.9 s.e.) lbs. The median duration of surgery was 50 minutes (range 18 to 125 min.). The median number of teeth extracted was 4 (range 2 to 4), and the median DSD was 8 (range 3 to 12).
Anesthetic medications used for intravenous moderate or deep sedation routinely included an opioid (fentanyl, alfentanil, or sufentanil) and sedatives (propofol and/or midazolam). For the majority of the anesthetic regimens, an anti-emetic (odansetron), a long-acting local anesthetic (bupivacaine), and an anti-inflammatory steroid (dexamethasone) were additionally administered.
On the day following surgery, the participants described the worse pain they had experienced as none (5), mild (19), moderate (14), and severe (10). During days 2 to 7, worse pain was reported as none (4), mild (10), moderate (18), and severe (9). At the time of the 7-day postoperative interview, the majority of the patients described their existing discomfort as “pain free” (24 patients) or “mild pain discomfort” (nine patients) or “slight tenderness” (eight patients) (Table 1).
A prescription for an opioid combination analgesic (Vicodin®, Lorcet®, Percocet®, or Norco®) was prescribed to all of the patients. The median number of tablets prescribed was 20 (range 10 to 40). Two patients did not fill their prescriptions, and three patients took none of the opioids prescriptions that they had filled. One day following surgery, patients reported consuming a median of three tablets (range 0 to 10), and by 7 days, patients reported consuming a total of a median of eight tablets (range 0 to 34). The remaining unused opioid analgesics tablets (median = 12) were reported to be stored in medicine cabinets (22 patients), purses (four patients), drawers (three patients), “mom’s room” (two patients), nightstands (one patient), suitcase (one patient), child-safe medicine cabinet (one patient), or unknown/not filled (seven patients). None of the patients reported discarding their unused opioid prescriptions. Peripherally acting analgesics, including ibuprofen (30 patients), acetaminophen (six patients), naproxen (two patients), and combinations of acetaminophen and ibuprofen (two patients), were reportedly used throughout the 7-day recovery period.
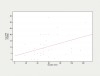
It was determined through statistical modeling using multiple regression analysis that the total opioid analgesic consumption was not related to patient characteristics (age, weight, gender), anesthetic and adjunctive agents, or surgical difficulty. The only variable found to correlate with OPR consumption during the 7-day postoperative experience was the duration of the surgical procedure (P = 0.0297) (Figure 1).
Complete amnesia to the local anesthetic administration was reported by all 48 patients. Lack of recall for the surgical extraction procedure was reported by 46 of the 48 patients (96%). Nausea/vomiting was reported during the 1-day interview by four patients, and six patients reported nausea/vomiting during the following 6 days of recovery. Other reporting adverse events included two patients with prolonged bleeding/oozing reported during the first-day interview, and two patients also reported soreness at the venipuncture site during the first day. No intervention was required for either the bleeding from the extraction site or venipuncture soreness. One patient returned 5 days following surgery for treatment of an apparent localized alveolar osteitis (dry socket), and one patient continued to have pain and swelling at 7 days that was believed to be a soft-tissue infection; both of these patients were prescribed additional opioid analgesics.
Discussion
Because the young adult patient population used in this assessment was recruited from a dental school clinic in an urban setting, the findings may not be generalizable to other settings. Surgical residents early in their training performed many of the surgeries. This surgical variable can be noted by the broad range of surgical durations (18 to 125 minutes) seen in Figure 1. The anesthetic and adjunctive agents used, although not uncommon, may not reflect the sedation and anesthesia practices provided in private practitioners’ offices or other settings. The regimen of anesthetic and adjunctive agents used in the authors’ clinic for these surgical procedures were quite similar, limiting their ability to assess specific drug-related complications.
The most severe pain reports occurred during the first days following surgery and diminished throughout the 7-day postoperative period, with the majority of patients reporting to be essentially “pain free” after 1 week. The long-acting local anesthetic bupivacaine and anti-inflammatory steroid dexamethasone were routinely administered to limit postoperative swelling, trismus, and discomfort. A pre-emptive nonsteroidal anti-inflammatory drug (NSAID), usually naproxen, was provided to 21 of the patients. NSAIDs and acetaminophen were recommended as the primary analgesics for managing postoperative pain.4,5
Four patients reported nausea and/or vomiting during the first day, with a total of eight patients reporting nausea and/or vomiting during the entire 1-week recovery period (two patients reported nausea/vomiting at both interviews). The incidence may be somewhat higher than previously reported because the patients were specifically asked about this complication. As a routine within the Department of Dental Anesthesiology, most of the 48 patients participating in this assessment received both dexamethasone (91.6%) and odansetron (81.3%). Both of these agents are believed to limit postoperative nausea and vomiting; six of the eight patients who experienced nausea and vomiting had received these antiemetic agents.6,7 It is interesting to note that the nausea and vomiting often occurred beyond the first 24-hour period, suggesting that this complication may be due as much to the OPRs as to a complication of the anesthetic drugs or surgical procedure.
An opioid prescription for 20 tablets was found to adequately manage expected postoperative pain. Two patients with painful post-surgical infections and one patient whose surgical procedures lasted more than 90 minutes required additional opioid combination analgesic. Apparently, a prescription for 20 tablets is usually sufficient to manage acute postoperative pain if recovery follows a normal healing process. Larger prescriptions of OPRs may encourage patients to rely on opioids for pain relief instead of returning to the clinic to receive proper professional follow-up treatment that may be indicated.
It is interesting to note that five (10%) patients having undergone third-molar extractions took none of the prescribed OPR.
Because of the concern for misuse of prescription OPRs (most notably Vicodin®), oral and maxillofacial surgeons in the United States have increased their reliance on preventative strategies that may limit pain severity and delay its onset. These strategies include the use of long-acting local anesthetics and systemic glucocorticosteroids, practices that appear to have increased in the last decade.2,8-13 Many practitioners will additionally provide a peripherally acting agent (such as ibuprofen or naproxen) prior to surgery to limit the severity of postoperative pain.2,8,14,15 Postoperative pain management using the combination of a NSAID and acetaminophen provides an additional strategy for pain management that does not rely on OPRs.16-18
The authors’ analysis of potential predictors of patient OPR consumption was limited by the small sample of patients evaluated. Age and weight were not found to be reliable predictors. There was a trend, although statistically non-significant, showing increased consumption of OPRs among the female patients (males = 8.1 tablets vs. females = 11 tablets). Combining all potential risk factors found that only the duration of surgery predicted an increased consumption of OPRs during the entire 7-day recovery period following surgery. The duration of surgery appears to be inclusive of several risk factors, including number of teeth, surgical trauma, and surgeon’s experience. Each of these factors is likely to increase a patient’s postoperative pain experience.
The location and storage of the prescribed OPR medications was varied, with only one patient reporting that his prescription was kept in a locked childproof cabinet. Because these medications are being administered to adolescents and young adults, improved patient and parent education is recommended to assure that these potentially hazardous medications are securely stored to prevent misuse or abuse.3,19,20 Specific instructions for secure storage, not sharing, and proper disposal should be established by all practitioners providing prescriptions for OPRs.
Conclusions
A postoperative telephone survey found that a prescription for 20 tablets of an opioid-containing pain reliever was adequate for 95% of studied patients who had undergone third-molar extractions. Moderate-to-severe pain during the first days following surgery diminished throughout the 7-day postoperative period. Five patients took none of the prescribed OPR tablets, and two patients, who had developed post-extraction infections, found the initial prescription of 20 tablets to be inadequate. Future research will address effective alternatives to opioid analgesics and effective strategies to improve patient education regarding the safe storage and disposal of unused prescription opioid-containing analgesics.
Disclosure
The authors had no disclosures to report.
Funding of this project was sponsored entirely by the Department of Dental Anesthesiology at the University of Pittsburgh School of Dental Medicine.
Acknowledgement
Preliminary results were previously presented: Weiland B, Wach A, Kanar B, Sosovicka M, Cooke M, Moore P. Postoperative Pain, Prescription Analgesic Use and Complications Following Third Molar Extractions. America Dental Society of Anesthesiology Annual Session, April 26-28, 2013.
About the Authors
Breanna M. Weiland, DMD
Resident, Division of Dental Anesthesiology, Department of Anesthesiology, Stony Brook University School of Dental Medicine, Stony Brook, New York
Anthony G. Wach, DMD
Resident, Department of Dental Anesthesiology, University of Pittsburgh School of Dental Medicine, Pittsburgh, Pennsylvania
Brent P. Kanar, DMD
Resident, Department of Dental Anesthesiology, University of Pittsburgh School of Dental Medicine, Pittsburgh, Pennsylvania
Matthew T. Castele, DMD
Resident, Department of Dental Anesthesiology, University of Pittsburgh School of Dental Medicine, Pittsburgh, Pennsylvania
Mark F. Sosovicka, DMD
Assistant Professor, Department of Oral and Maxillofacial Surgery, University of Pittsburgh School of Dental Medicine, Pittsburgh, Pennsylvania
Matthew R. Cooke, DDS, MD, MPH
Assistant Professor, Department of Dental Anesthesiology, University of Pittsburgh School of Dental Medicine, Pittsburgh, Pennsylvania
Paul A. Moore, DMD, PhD, MPH
Professor, Department of Dental Anesthesiology, University of Pittsburgh School of Dental Medicine, Pittsburgh, Pennsylvania
Queries to the author regarding this course may be submitted to authorqueries@aegiscomm.com.
References
1. Moore PA, Nahouraii HS, Zovko JG, Wisniewski SR. Dental therapeutic practice patterns in the U.S. I: Anesthesia and sedation. Gen Dent. 2006;54(2):92-98.
2. Moore PA, Nahouraii HS, Zovko JG, Wisniewski SR. Dental therapeutic practice patterns in the U.S. II. Analgesics, corticosteroids, and antibiotics. Gen Dent. 2006;54(3):201-207.
3. Oakley M, O’Donnell J, Moore PA, Martin J. The rise in prescription drug abuse: raising awareness in the dental community. Compend Contin Educ Dent. 2011;32(6):14-22.
4. Derry C, Derry S, Moore RA, McQuay HJ. Single dose oral naproxen and naproxen sodium for acute postoperative pain in adults. Cochrane Database Syst Rev. 2009;21(1):doi: 10.1002/14651858.CD004234.pub3.
5. Hersh EV, Moore PA, Ross GL. Over-the-counter analgesics and antipyretics: a critical assessment. Clin Ther. 2000;22(5):500-548.
6. Henzi I, Walder B, Tramer MR. Dexamethasone for the prevention of postoperative nausea and vomiting: a quantitative systematic review. Anesth Analg. 2000;90(1):186-194.
7. Tramer MR, Reynolds DJ, Moore RA, McQuay HJ. Efficacy, dose-response, and safety of ondansetron in prevention of postoperative nausea and vomiting: a quantitive systemic review of randomized placebo-controlled trials. Anesthesiology. 1997;87(6):1277-1289.
8. Moore PA, Brar P, Smiga ER, Costello BJ. Preemptive rofecoxib and dexamethasone for prevention of pain and trismus following third molar surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;99(2):E1-E7.
9. Misch CE, Moore P. Steroids and the reduction of pain, edema and dysfunction in implant dentistry. Int J Oral Implantol. 1989;6(1):27-31.
10. Truollos ES, Hargreaves KM, Butler DP, Dionne RA. Comparison of non-steroidal anti-inflammatory drugs, ibuprofen and flurbiprofen, to methylprednisolone and placebo for acute pain, swelling, and trismus. J Oral Maxillofac Surg. 1990;48(9):945-952.
11. Gordon SM, Brahim JS, Dubner R, et al. Attenuation of pain in a randomized trial by suppression of peripheral nociceptive activity in the immediate postoperative period. Anesth Analg. 2002;95(5):1351-1357.
12. Moore PA. Bupivacaine: a long-lasting local anesthetic for dentistry. Oral Surg Oral Med Oral Pathol. 1984;58(4):369-374.
13. Moore PA. Long-acting local anesthetics: a review of clinical efficacy in dentistry. Compendium. 1990;11(1):22-30.
14. Dionne RA, Cooper SA. Evaluation of preoperative ibuprofen for postoperative pain after removal of third molars. Oral Surg Oral Med Oral Pathol. 1978;45(6):851-856.
15. Jackson DL, Moore PA, Hargreaves KM. Preoperative nonsteroidal anti-inflammatory medication for the prevention of postoperative dental pain. J Am Dent Assoc. 1989;119(5):641-647.
16. Moore PA, Hersh EV. Combining ibuprofen and acetaminophen for acute pain management after third-molar extractions: translating clinical research to dental practice. J Am Dent Assoc. 2013;144(8):898-908.
17. Hyllested M, Jones S, Pedersen JL, Kehlet H. Comparative effect of paracetamol, NSAIDs or their combination in postoperative pain management: a qualitative review. Brit J Anaesth. 2002;88(2):199-214.
18. Hersh EV, Kane WT, O’Neil MG, et al. Prescribing recommendations for the treatment of acute pain in dentistry. Compend Contin Educ Dent. 2011;32(3):22-30.
19. Golubic S, Moore PA, Katz N, et al. Opioid prescribing in dentistry: trends, ethical considerations, and diversion and abuse prevention. Inside Dentistry. 2011;7(6):50-60.
20. Denisco RC, Kenna GA, O’Neill MG, et al. Prevention of prescription opioid abuse: the role of the dentist. J Am Dent Assoc. 2011;142(7):800-810.